Abstract
Bell’s palsy is the most common mononeuropathy that causes acute unilateral facial paralysis or paresis. The condition peaks within 72 h and may be associated with numerous signs and symptoms, including post-auricular pain, drooping of the eyelid, loss of taste sensation and decreased lacrimation. Although the etiology of the condition is unknown, inflammation, viral infection, ischemia and anatomy of the facial nerve have all been implicated in the pathophysiology of the disease. Diagnosis and determination of etiology are significant in the early management of this condition. Most incidents resolve spontaneously; however, treatment reduces cases of incomplete recovery and entails the use of corticosteroids, with a possible role for antivirals if a viral etiology is suspected. For patients with incomplete recovery, long-term complications have esthetic, physiological and psychological implications, which greatly affect their quality of life. The purpose of this article is to summarize the current literature on etiology, diagnosis and management of Bell’s palsy.
Idiopathic facial nerve paralysis, commonly known as Bell’s palsy (BP), is a cranial nerve VII condition leading to facial weakness (paresis) or paralysis. This acute unilateral paralysis or paresis has no identifiable cause and occurs over <72 h.1 BP has been alluded to numerous times throughout history, with descriptions of the condition found in ancient Greek, Persian and European medical texts dated as early as the 5th century BCE.2,3 Ancient Peruvian ceramic art, Razi’s “al-Hawi” and the Greek Hippocrates all indicate familiarity of these ancient cultures with BP.2–4 Many physicians throughout history, including Sydenham, Friedreich, Stalpart van der Wiel and Thomassen á Thuessink, have researched and described the condition.2,3 The name comes from Sir Charles Bell, a surgeon, who took great interest in sensory (trigeminal nerve) and motor (facial nerve) innervation of the face.2,5
Signs and symptoms of BP include ipsilateral drooping of the eyelid, dry eye, excessive tearing, drooping of the corner of the mouth, post-auricular pain, loss of taste sensation in the anterior 2 thirds of the tongue, difficulty eating, dry mouth, slavering, altered sensation and hyperacusis.2,6 The most pathognomonic sign of BP is the Bell’s phenomenon, characterized by upward rolling of the eye when attempting to close the eyelid.7 Figure 1 illustrates the most common clinical signs of BP.
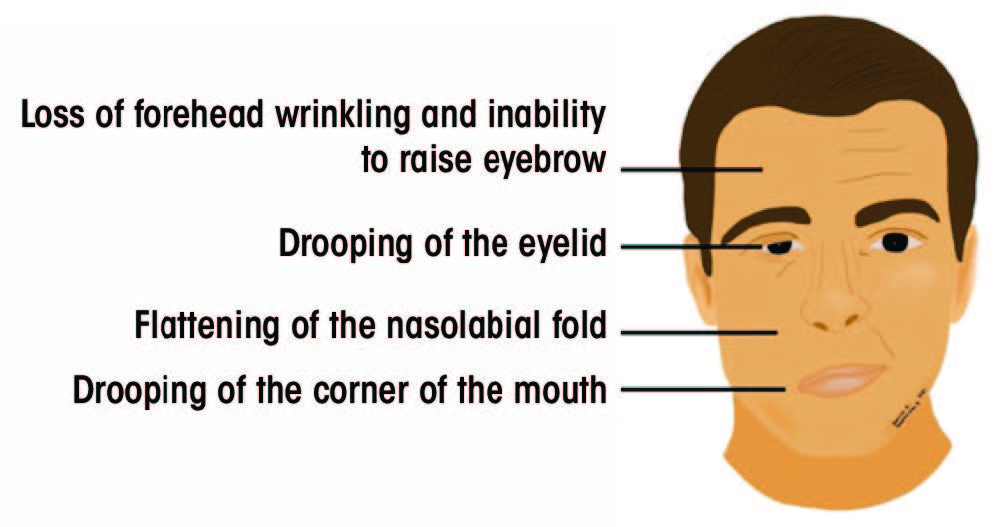
Figure 1: Signs of acute unilateral Bell’s palsy
Although the etiology of BP is unclear, most cases resolve without treatment.6 Short-term consequences of BP include the inability to close the eye, potential cornea injuries and eventual eye dryness, which can be managed clinically with a favourable prognosis.1 Long-term, incomplete recovery from BP can result in facial asymmetry, disfigurement, reduced facial movement and many other complications that greatly reduce the patient’s quality of life.1,8,9 Although various modalities are available to improve quality of life, patients with BP often experience depression, reduced quality of interpersonal relations, anxiety, decreased self-esteem and social isolation.10–12 This article aims to discuss the current evidence for the etiology, diagnosis and treatment of BP and its implications in the field of dentistry.
Epidemiology
BP is the most common cranial mononeuropathy with a reported incidence rate of 11.5–40.2 per 100 000.2,13 It is seen equally in males and females and occurs in all ages with a propensity to affect people in mid to later life.14 No race predilection exists, and both sides of the face are equally affected, although bilateral BP is rare (0.3% of cases).2,15 Various epidemiological studies have established a seasonal trend, with higher incidence in colder months of the year.2,16 Even without treatment, 70% of affected people will have complete resolution, while approximately 30% will experience partial or incomplete recovery.17 The recurrence rate of BP is estimated to be 7% and does not correlate with the prognosis.14,18 Recurrence should alert the clinician to alternative causes of facial paralysis.14 Possible risk factors for BP include hypertension, severe preeclampsia, psychological concerns, pregnancy, radiation exposure, diabetes, obesity, upper respiratory infection and migraine.1,19 Numerous cases of BP have been documented following the administration of influenza vaccines as well as many others.20 Similarly, recent studies have identified BP as a side effect of the new mRNA SARS-CoV-2 vaccine.21-23
Cranial Nerve VII Anatomy
Cranial nerve VII is a multifunctional nerve with significant motor, sensory and parasympathetic activities. Its nerve fibres are associated with 3 nuclei in the medulla oblongata and the pons: solitary (sensory), facial (motor) and superior salivatory (parasympathetic).24 The central motor nucleus of the facial nerve is located in the precentral gyrus of the motor cortex.25 Fibres from the central motor nucleus travel down in the corticobulbar tracts and supply the contralateral facial nucleus.25
The facial nerve is divided into 6 segments: cisternal, meatal, labyrinthine, tympanic, mastoid and extracranial.25,26 The cisternal segment includes the motor root and the nerve of Wrisberg, which advance to the internal acoustic meatus.25,26 At the meatus, these nerve segments unite to form the meatal portion of the facial nerve.25–27 Throughout the cisternal and meatal paths, CN VII travels with the vestibulocochlear cranial nerve (VIII).25–27 Further, the labyrinthine portion extends from the cochlea to the vestibule of the inner ear and joins the geniculate ganglion.25–27 The tympanic portion runs inferior to the lateral semicircular canal and gives rise to the mastoid segment of the facial nerve.25–27 The mastoid segment exits the skull through the stylomastoid foramen and becomes the extracranial portion of the nerve.25–27 This portion gives rise to the digastric and posterior auricular nerves and advances through the parotid gland to give rise to the terminal branches.25–27
Each segment gives rise to various branches (Table 1).25–28 Understanding the function of these branches is extremely helpful in determining the location of the pathology along the facial nerve. Figure 2 depicts structures innervated by the facial nerve, as well as the superficial extracranial branches.
|
Facial nerve segments |
Branches |
Function |
|---|---|---|
| Cisternal | ||
| Meatal | ||
| Labyrinthine (including geniculate ganglion) | Greater superficial petrosal |
|
| Lesser petrosal |
|
|
| External petrosal |
|
|
| Tympanic | ||
| Mastoid | Stapedius |
|
| Chorda tympani |
|
|
| Nerve from auricular branch of vagus |
|
|
| Extracranial | Posterior auricular |
|
| Digastric |
|
|
| Stylohyoid |
|
|
| Temporal |
|
|
| Zygomatic |
|
|
| Buccal |
|
|
| Marginal mandibular |
|
|
| Cervical |
|
|
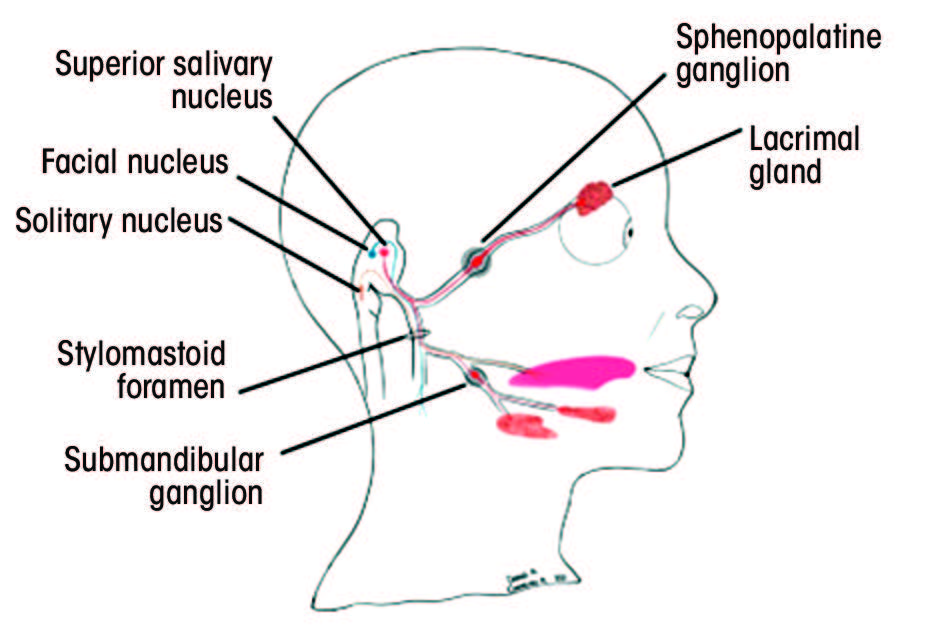
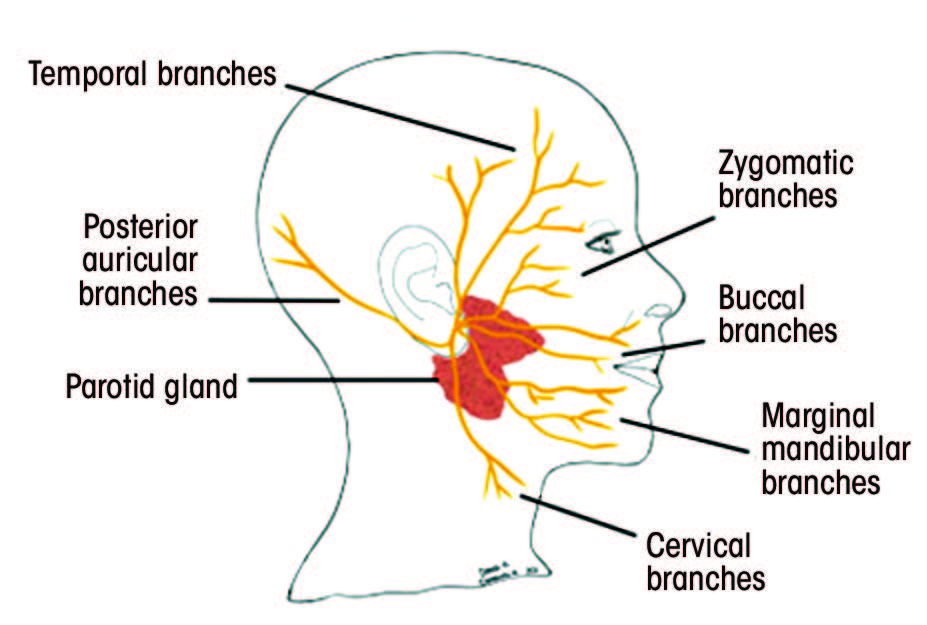
Figure 2: A. Structures innervated by the facial nerve. The red (parasympathetic), blue (motor) and orange (sensory) lines demonstrate the multifunctionality of the facial nerve. B. Superficial branches of the extracranial portion of the facial nerve.
Supranuclear pathology, more commonly known as upper motor neuron (UMN) palsy, results when neuronal fibres above the facial nucleus are disrupted.14,25 UMN palsy affects the contralateral half of the lower face, sparing the forehead and the eyebrow muscles.25 A UMN lesion of the cortex and/or corticobulbar tract spares the lacrimal and salivary secretions, and the taste function is preserved.29 Infranuclear pathology or lower motor neuron (LMN) palsy results from lesions at the facial nucleus or the exiting fascicles.29 These lesions affect the ipsilateral upper and lower face.14,25 Therefore, involvement of the forehead muscle (i.e., frontalis) and the eyebrow muscle (i.e., corrugator supercilii) provides insight into the nature of the condition. The sparing of the forehead and eyebrow muscles is attributed to the bilateral innervation of the upper third of the face and contralateral innervation of the lower 2 thirds.26 Precise location of an LMN palsy can be discerned via functional assessment of other neighbouring structures. LMN palsy involving the facial nucleus or the fascicles within the brainstem may exhibit contralateral hemiparesis, ataxia, nystagmus and CN III–CN VI palsy, as well as ophthalmoparesis.29 Conversely, LMN palsy involving the facial nerve after it exits from the brainstem may display complete ipsilateral hemifacial weakness, dysgeusia and a decrease in lacrimation and salivation.29
Etiology
The precise etiology of BP is unknown, and its diagnosis is based on exclusion.19 Consequently, it is essential to eliminate all other potential etiologies of facial paralysis and paresis before diagnosing BP. Currently, there are numerous theories regarding the cause of BP.19
Anatomy
The anatomy of the facial nerve and its long intra-bony path have been considered as potential factors in the etiology of BP. The fallopian canal is a narrow Z-shaped canal in the temporal bone.25 Although it provides protection to the facial nerve, it predisposes the nerve to entrapment neuropathies following inflammation or edema.30 The labyrinthine segment of the facial nerve is the narrowest portion of the canal,25 and the meatal foramen—the entry point of the nerve into the labyrinthine segment—is only ~0.68 mm in diameter.30 Also, an arachnoid band of tissue around the lateral portions of the internal acoustic meatus further contributes to constriction of the area.30 Celik et al.31 showed that reduced width of the fallopian canal in the labyrinthine portion is a risk factor for BP. Similarly, Ozan and Arslan32 found increased cross-sectional area of the facial nerve and decreased cross-sectional area of the internal acoustic meatus associated with BP. Therefore, compression of the facial nerve caused by inflammation or edema along its narrow intra-bony path may cause facial nerve abnormalities.
Viral Infection
Viral infection is hypothesized to be another etiological factor in BP.19 Varicella zoster virus (VZV) and herpes simplex virus (HSV) are DNA viruses that remain dormant in nervous ganglia subsequent to primary infection.33 They can reactivate anytime throughout the host’s lifespan and cause recurrent infections.33 In particular, HSV-1 remains latent in the geniculate ganglion of the facial nerve.33 Various studies have demonstrated the presence of HSV-1 DNA in the endoneural fluid of the facial nerve in BP patients, as well as the ability of HSV-1 to cause facial paralysis in animal models.34,35 Currently, HSV-1 mediated inflammation of the facial nerve in the narrow fallopian canal is widely accepted to be the mechanism responsible for most BP cases.30 Reinfection by VZV is also possible and more severe than HSV-1 because of its spread via satellite cells.30 A possible biomolecular mechanism of HSV-mediated neuronal dysfunction involves abnormal expression of p53 upregulated modulator of apoptosis (PUMA) and the innate immune signaling molecule, SARM1.19
Ischemia
The outer layer of the facial nerve consists of a periosteal membrane overlying a vascular plexus coating the epineurium of the facial nerve.36 This vascular plexus is supplied by the stylomastoid artery peripherally, with central layers supplied by the middle meningeal artery (petrosal branch), internal auditory artery and anterior inferior cerebral artery.19,24 Primary ischemia can result from vasospasms, leading to facial nerve neuropathy.19,36 Although this type of ischemia is rare, it can be appreciated in cases of diabetes mellitus and embolization of the middle meningeal artery.36 Quickly following acute ischemia, inflammation of the nerve begins with recruitment and activation of macrophages.19 Primary ischemia is also observed in animal models, with facial nerve paralysis occurring 5–15 minutes after blockage of the vascular network.37
Secondary ischemia is a consequence of primary ischemia, with initial constriction of the arterioles and subsequent dilation of the capillaries leading to production of a transudate.19,36 This transudate can compress the lymphatic capillaries, further increasing transudate production and inducing ischemia.19,36 The resultant histamine-mediated edema can lead to obstruction of venous outflow and, thus, interfere with normal arterial circulation in the vascular plexus.19,36 Secondary ischemia can progress to tertiary ischemia, where perivasculitis and endarteritis are evident.19,36 Thickening or fibrosis of the facial nerve sheath are often observed at this stage and may require surgical decompression to prevent permanent facial paralysis.36
Inflammation
Recently, more evidence has emerged regarding BP and inflammation‑induced demyelination of the facial nerve.19 Numerous studies have shown the association of a potential new marker—neutrophil to lymphocyte ratio (NLR)—with various inflammatory diseases, such as systematic lupus erythematous and hepatitis B.38,39 Similarly, a meta-analysis40 concluded that the NLR for patients with BP was higher than in patients without BP, and a higher NLR coincided with a worse prognosis. This indicates a change in the peripheral subpopulation of white blood cells as in other inflammatory demyelinating diseases, such as multiple sclerosis and Guillian-Barre syndrome.41–43 Other studies have demonstrated the role of cell-mediated immunological responses, with BP patients having higher serum levels of IL-6, IL-8 and TNF-a compared with controls.44
Management
Diagnosis
Thorough clinical examination and medical history are essential in diagnosing BP.45 Laboratory and imaging techniques are not routinely required, but suspicion of neoplasms, prolonged facial palsy episodes, hypoacusis, nystagmus, tinnitus, sensory deficits and diplopia should be investigated further using CT scans and MRI.45,46 Sufficient clinical suspicion of Lyme disease and varicella zoster oticus demand serological work up.1,46 Electromyography (EMG) is a useful tool in determining the extent of axonal damage, thus guiding treatment.45 Electroneurography (ENG) and EMG can also be used as a prognostic indicator, determining the signs and extent of facial nerve reinnervation.46,47 It has been recommended that electrodiagnostic testing for BP cases be limited to those with complete paralysis only, as the risk of incomplete recovery is higher for such patients.1
Patient history should include a description of the onset of facial palsy, as a progressive, slowly occurring facial palsy is indicative of a neoplastic or infective etiology.48 It should be noted that the onset of BP is sudden and tends to worsen over minutes to hours.48 Alternative pathologies, including neurologic, otologic, trauma, inflammatory and congenital abnormalities, should also be excluded.28
Physical examination should include close inspection of the facial muscles with emphasis on the eyelids, nasolabial folds and the corners of the mouth.28 In BP, incomplete closure of the eyes, weakness of the orbicularis oculi muscle leading to Bell’s phenomenon (i.e., palpebral-oculogyric reflex) and lagging blink of the affected side are common.28 In addition, patients may exhibit difficulty in puffing out cheeks and pursing their lips.28 Examining taste senses using a tongue blade and salt/sugar could also assist in the diagnosis.28 Finally, the orbicularis oculi reflex test and the corneal reflex test may be conducted. The former involves gently tapping the glabella to observe involuntary blinking reflex, while the latter is carried out by stimulating the cornea with a wisp of cotton.28
Clinical practice guidelines by Baugh et al.1 provide certain criteria for diagnosing BP (Figure 3). A clinical examination algorithm for the diagnosis of BP is described in Figure 4.48 Currently, the degree of facial paralysis is determined via the House-Brackmann scale,49 which assesses various facial attributes including symmetry in rest and movement. This scale is divided into 6 grades, with a higher grade associated with a greater severity of BP and a more incomplete recovery (Table 2).49
|
Grade |
Symptoms |
|---|---|
| I |
|
| II |
|
| III |
|
| IV |
|
| V |
|
| VI |
|
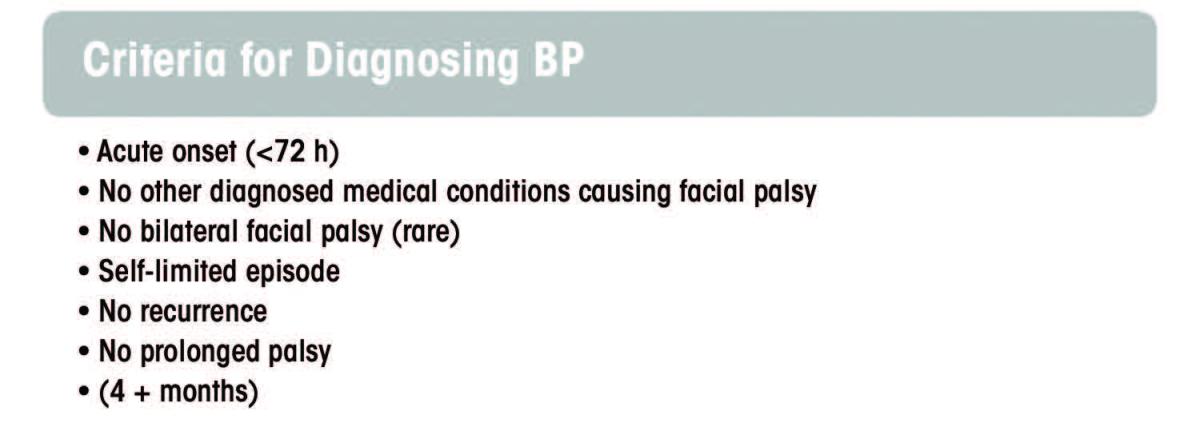
Figure 3: Criteria for diagnosing BP

Figure 4
Various signs and symptoms may prompt the clinician to consider an alternative diagnosis. These include severe pain, hearing or vestibular abnormalities (excluding hyperacusis), history of cancer, prior insect bite and rash in or around the ear.46,50 The rate of misdiagnosis of BP is approximately 10.8%.2,5,14 The literature suggests misdiagnosis rates of up to 24% with central and secondary peripheral pathologies, such as skull base tumours being misinterpreted as BP.29 Table 3 shows conditions and syndromes that may result in facial paralysis and/or paresis.1,14,46,50 Table 4 highlights some specific examination findings that would assist in ruling out other important entities in the differential diagnosis.28
|
Differential diagnosis |
Conditions |
|---|---|
| Parenchymal lesions |
|
| Trauma |
|
| Neoplasms |
|
| Congenital |
|
| Meningitis |
|
| Infection |
|
| Neuromuscular junction disorders/myopathy |
|
| Endocrine |
|
| Neurovascular |
|
| Other |
|
|
Condition |
Defining characteristics |
|---|---|
| Cerebrovascular event (e.g., stroke) |
|
| Guillain-Barre syndrome |
|
| Diabetes mellitus |
|
| Infection (e.g., meningitis and encephalitis) |
|
| Lyme disease |
|
| Ramsay Hunt syndrome |
|
| Sarcoidosis |
|
| Neoplasms (e.g., parotid tumour) |
…

|