Abstract
Introduction:
Views on silver diamine fluoride (SDF) have been studied in various settings worldwide but remain underexplored in the Canadian context. In this study, we explored awareness, acceptability, general and economic perception and potential patient acceptance of SDF for caries management in children and older adults. We also looked at the impact of an educational workshop on SDF for dental professionals in Northern Ontario.
Methods
A 42-item structured questionnaire was administered to attendees at a workshop on minimally invasive dentistry held in Thunder Bay, Ontario. It elicited information regarding respondents’ demographics, their perception, acceptance and use of SDF and the workshop’s influence on uptake of the material.
Results:
Participants in this cross-sectional study were 53 dental professionals, mainly dental hygienists (45.3%) and dentists (35.8%). Their views on the use of SDF as a minimally invasive technique and on how it was accepted by their patients and patients’ caregivers were generally positive. Respondents reported that the workshop made them more likely to choose SDF for treating children (82.4%) and older adults (87.8%). We noted differences between dentists and non-dentists, specifically regarding potential parental acceptance of SDF staining in anterior temporary teeth (p = 0.030), as well as SDF’s benefits in older adults in long-term care (p = 0.007), with a higher proportion of non-dentists viewing SDF more favourably.
Conclusions:
SDF awareness and acceptance were high among dental professionals in Northern Ontario who attended a workshop presenting the beneficial effects of SDF for children and older adults.
Introduction
Over 7 years have passed since Health Canada approved 38% silver diamine fluoride (SDF) as a dental caries arresting agent.1 This came on the heels of the United States’ Food and Drug Administration’s endorsement in 2014.2 Provider, patient and research interest in SDF has been on the rise ever since.3,4 Since its approval by Health Canada in 2017, particular attention has been paid to studying the advantages of using SDF’s caries arrest effects in children and older adults (≥65 years) as its 38% presentation (that is containing 44 800 ppm of fluoride) is considered a “patient” and “operator” friendly minimally invasive, non-aerosol generating procedure.4,5 In pediatric dentistry, interest in SDF lies in the avoidance of pharmacologic behaviour guidance techniques,6 its application in public health settings7 and its potential cost-effectiveness.8,9 In older adults, it has been suggested as advantageous in root caries10 and dentin hypersensitivity11 management.
Despite evidence of SDF’s uses and advantages, its main drawback is the staining that develops on any demineralized surface it touches. Worldwide, this has been reported to be a point of resistance towards SDF’s use among parents,12 dental professionals13 and some authorities and decision-makers.14,15
In the Canadian context, literature on SDF is scarce. Parents whose children were treated with SDF for severe early childhood caries (ECC) in Manitoba were satisfied with the treatment but desired more guidance and education about the material.16 First Nations and Métis parents (also in Manitoba) similarly reported being open to the treatment, if adequate information was provided beforehand.17 On the education front, a 2018 survey of Canadian dental and dental hygiene programs revealed that SDF use is taught didactically in most programs (93%), but in a lower proportion clinically.18 We found no studies in the literature on the perception of SDF among Canadian dental professionals.
In Canada, SDF could play a beneficial role in caries management. Over a third (38.9%) of Canadian children 1-9 years of age have untreated caries lesions in their temporary teeth.19 This figure is exacerbated in Indigenous children: both the 2009–2010 First Nations Oral Health Survey20 and the 2018 First Nations Regional Health Survey21 revealed disparate outcomes in the oral health of Indigenous children compared with their non-Indigenous counterparts. In older adults, rates of root decayed or filled teeth have been reported to be 43.3% among dentate Canadians aged 60–79 years. 22 These data suggest that, in Canada, children, seniors in long-term care (LTC), Indigenous people, new immigrants, special needs individuals and people with low income are the populations most at risk for developing dental caries.23
Furthermore, health services delivery becomes more challenging in small towns and regions not adjacent to metropolitan areas24,25; this speaks to the structural barriers that exist in delivering and accessing care across the country. Canadian cities and towns that are regional hubs play important roles in commerce, cross-country connectivity and health services. For example, Thunder Bay is a key hub in northwestern Ontario, with its diverse population and close ties to Indigenous peoples in the area and surrounding Treaty lands.26 Thunder Bay is home to multiple health care facilities that provide necessary care and educational centres that train valuable professionals for the region. Although inhabitants of northwestern Ontario have typically traveled to such hubs to receive care, important shifts, like those led by Indigenous Health Transfer initiatives, are permitting self-governance and facilitating access to care to people who have historically been underserved.27
More can be done to strengthen the oral health care capacity in this important region. If the benefits of SDF are to be reaped and its adequate adoption pursued in Thunder Bay and similar regions, dental professionals’ perceptions of the material and potential barriers to its use must be understood. Therefore, this study aimed to analyze the awareness, acceptability among professionals, their general and economic perceptions and potential patient acceptance of SDF for caries management in children and older adults, as well as the impact of an educational workshop among dental professionals in Northern Ontario.
Methods
Study Design: Setting and Participants
We carried out this descriptive cross-sectional study in Thunder Bay, Ontario, on 17 November 2023. Participants were dental professionals who voluntarily completed a questionnaire after attending an in-person continuing education workshop titled: Be SMART: Improve Your Practice with Silver Diamine Fluoride and Glass Ionomer Cement. Dental professionals were viewed as any person who serves populations in the area of oral health care in any capacity (general practitioners, dental specialists, dental hygienists, dental educators, etc.).
An invitation to the workshop was extended to dental professionals in Thunder Bay and surrounding areas, including First Nations communities. It was led by an experienced American-board-certified pediatric dentist with expertise in minimally invasive dentistry. Workshop topics included the use of SDF for children and older adults, the use of glass ionomer cement restorations and the use of combined techniques, also known as SMART: silver modified atraumatic restorative technique.
After the workshop, participants were asked to complete a questionnaire, assisted but not guided by the research team. Written consent was obtained before attendees answered the questionnaire, and their participation (or lack thereof) did not affect their participation or credit for the workshop in any way. Participant anonymity was maintained throughout the study, no names were attached to the study instrument. Data analysis took this a step further by assigning participant identification numbers. Participants did not receive compensation for completing the questionnaire, and attendance at the workshop was free of charge. The workshop was advertised by Confederation College Thunder Bay, the Thunder Bay Dental Association and the Thunder Bay Dental Hygienists’ Society.
Questionnaire Design
The survey instrument was based on the aims of the study, previous literature on the topic (perceptions of SDF) and the investigators’ expertise (HPL: dental public health, KST: economic evaluations and FAP: pediatric dentistry). After a thorough literature review, expert consideration and taking into account research experience in the region, the authors concluded that existing surveys did not capture important topics related to the population and setting sampled, nor did they address some of the objectives in this study (e.g., decision-making in remote communities, cost perception and use of SDF in LTC).
Thus, a new instrument was constructed. The questionnaire included 42 items divided into 3 sections. The first part collected information regarding characteristics of the dental professionals and their patients. The second gauged participants’ general perceptions of SDF use, the perceived acceptability of SDF for their patients, perceptions of SDF’s effectiveness, costs and accessibility of SDF use in pediatric and older adult populations and the workshop’s influence on their SDF perceptions. Finally, 3 open-ended questions asked participants to report whether they perceived any additional problems (besides staining) in the acceptance of SDF for children and adults.
The instrument was developed in English and piloted with a similar cohort (dental professionals) before being administered to study participants. No content changes were made after piloting, only grammatical stylistic ones. The instrument can be made available on request to the corresponding author.
Data Analysis
Information collected in paper form was entered into the REDCap software (Vanderbilt University, 2004) to codify the data. Descriptive analysis was carried out to summarize the overall responses of participants. An exploratory subgroup analysis (Χ2 test) was then conducted to determine whether differences existed between dentists and non-dentist groups. In addition, an analysis of the effect of having received prior education on SDF regarding its uptake was also conducted (Χ2 test ). All data were analyzed using the SPSS statistical software package with significance set at p ≤ 0.05.
Ethics Approval
Prior ethics approval was received from the University of Toronto Research Ethics Board (RIS protocol no. 45469).
Results
Of 64 workshop attendees, 53 dental professionals aged 19–79 years (mean 45.9 years) completed the study questionnaire (Table 1). Most were dental hygienists (45.3%), followed by dentists (35.8%). The remainder of the participants included dental hygiene students, dental assistants and people who self-identified as “other,” which included health educator in combination with dental assistant or dental hygienist. Dental professionals who had been practising for ≥31 years were in the majority in this study (32.7%).
|
Characteristic |
No. (n = 53) |
% |
|---|---|---|
|
Note: CI = confidence interval. |
||
| Sex | ||
| Female | 38 | 71.7 |
| Male | 15 | 28.3 |
| Age, years | ||
| Mean (95% CI) | 45.9 (41.8–50.0) | |
| Median | 47 | |
| Standard deviation | 14.2 | |
| Range | 60 (19–79) | |
| Occupation | ||
| Student | 4 | 7.5 |
| Dental assistant | 2 | 3.8 |
| Dental hygienist | 24 | 45.3 |
| Dentist | 19 | 35.8 |
| Other | 4 | 7.5 |
| Specialization | ||
| Yes | 4 | 7.5 |
| No | 49 | 92.5 |
| Years in practice | ||
| 1–5 | 7 | 13.5 |
| 6–10 | 7 | 13.5 |
| 11–15 | 5 | 9.6 |
| 16–20 | 6 | 11.5 |
| 21–30 | 10 | 19.2 |
| ≥31 | 17 | 32.7 |
Participants reported serving different communities in and around Thunder Bay. Figure 1 depicts the regional distribution of the cities or First Nations reserves that the participants serve. Almost all dental professionals (98.1%) reported serving Indigenous patients, with 13.7% claiming an Indigenous patient population of 75% or more (Table 2). For 76.9% of the participants, 25–50% of their patient population was pediatric, and for 73.1%, 25–50% were older adults.
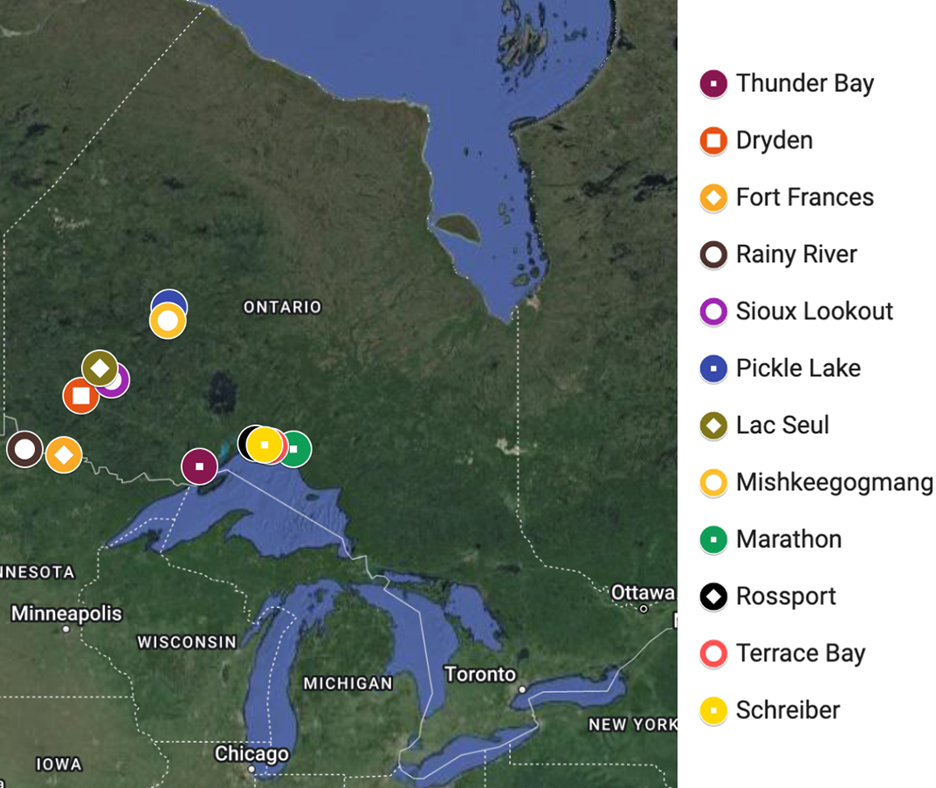
Figure 1: Cities served by workshop participants.
|
Characteristic |
% (n = 53) |
|---|---|
| Indigenous persons | |
| Yes | 98.1 |
| No | 1.9 |
| Proportion of Indigenous patients served | |
| 25% | 70.6 |
| 50% | 15.7 |
| 75% | 5.9 |
| 100% | 7.8 |
| Proportion of pediatric patients served (≤12 years old) | |
| 0% | 11.5 |
| 25% | 61.5 |
| 50% | 15.4 |
| 75% | 3.8 |
| 100% | 7.7 |
| Proportion of older adult patients served (≥65 years old) | |
| 0% | 9.6 |
| 25% | 40.4 |
| 50% | 32.7 |
| 75% | 15.4 |
| 100% | 1.9 |
All participants were aware of the use of SDF for pediatric patients before the workshop, but only 45.1% had received education on this topic as part of their professional training (Table 3). Most (88.7%) had heard of the use of SDF for older adults, and less than half (42.6%) received education on this use as part of their professional training.
Less than half of the study participants (43.4%) reported having previously used SDF in their clinical practice; 60.8% had never used it for pediatric patients and 57.7% had never used it with older adults (Table 3). Of those who reported having used SDF in older adults, nearly a third (32.1%) had used it for root caries, 30.2% for coronal caries and only 9.4% for dentin hypersensitivity.
|
Awareness of SDF |
% (n = 53) |
|---|---|
| Awareness of SDF use for pediatric patients before the workshop | |
| Aware | 100 |
| Not aware | 0 |
| Education on SDF use for pediatric patients as part of professional training | |
| Received | 45.1 |
| Not received | 54.9 |
| Awareness of SDF use for older adult patients before the workshop | |
| Aware | 88.7 |
| Not aware | 11.3 |
| Education on SDF use for older adult patients as part of professional training | |
| Received | 42.6 |
| Not received | 57.4 |
| Use of SDF | |
| Use of SDF in clinical practice | |
| Previously used | 43.4 |
| Never used | 56.6 |
| Frequency of SDF use in clinical practice | |
| Never | 55.8 |
| Rarely | 9.6 |
| Sometimes | 19.2 |
| Often | 11.5 |
| Very often | 3.8 |
| Frequency of SDF use for pediatric patients in clinical practice | |
| Never | 60.8 |
| Rarely | 9.8 |
| Sometimes | 19.6 |
| Often | 7.8 |
| Very often | 2.0 |
| Frequency of SDF use for older adult patients in clinical practice | |
| Never | 57.7 |
| Rarely | 11.5 |
| Sometimes | 19.2 |
| Often | 5.8 |
| Very often | 5.8 |
| Type of SDF use for older adult patients in clinical practice | |
| Root caries | |
| Checked | 32.1 |
| Unchecked | 67.9 |
| Coronal caries | |
| Checked | 30.2 |
| Unchecked | 69.8 |
| Dentin hypersensitivity | |
| Checked | 9.4 |
| Unchecked | 90.6 |
Most dental professionals had a positive view toward using SDF in children: they strongly agreed/agreed that they would use SDF to treat ECC in their community (84.9%) and that they would offer SDF treatments in cases where it could delay/prevent a child from having to be treated under general anesthesia (88.7%, Table 4).
|
Statement |
Response, % (n = 53) |
|---|---|
| Use | |
| I would use SDF to treat early childhood caries in my community | |
| Strongly disagree/disagree | 7.5 |
| Unsure | 7.5 |
| Strongly agree/agree | 84.9 |
| I would offer SDF treatments in cases where it could delay/prevent a child from having to be treated with general anesthesia | |
| Strongly disagree/disagree | 5.7 |
| Unsure | 5.7 |
| Strongly agree/agree | 88.7 |
| I have the option of using SDF for treatment in my practice | |
| Strongly disagree/disagree | 29.4 |
| Unsure | 15.7 |
| Strongly agree/agree | 54.9 |
| Acceptability | |
| Parents of my patient population would accept using SDF to treat early childhood caries. | |
| Strongly disagree/disagree | 1.9 |
| Unsure | 26.4 |
| Strongly agree/agree | 71.7 |
| Parents of my patient population would not accept SDF staining on posterior temporary teeth. | |
| Strongly disagree/disagree | 45.3 |
| Unsure | 30.2 |
| Strongly agree/agree | 24.5 |
| Parents of my patient population would not accept SDF staining on anterior temporary teeth. | |
| Strongly disagree/disagree | 15.1 |
| Unsure | 39.6 |
| Strongly agree/agree | 45.3 |
| Parents of my patient population would be more likely to accept SDF (in any sector) if their child had a previous early childhood caries treatment under general anesthesia. | |
| Strongly disagree/disagree | 7.5 |
| Unsure | 35.8 |
| Strongly agree/agree | 56.6 |
| Children of the population I serve would accept the SDF staining (in any sector). | |
| Strongly disagree/disagree | 15.1 |
| Unsure | 56.6 |
| Strongly agree/agree | 28.3 |
EFFECTIVENES…

| |