Modern dentistry should strive to preserve all maintainable natural teeth whenever possible, in line with the principles of minimal invasiveness and biological respect. However, in certain clinical scenarios, particularly when the remaining dentition is compromised by periodontal disease, periapical pathology and questionable long-term prognosis, full-arch rehabilitation with dental implants may represent a pragmatic, patient-driven alternative.
The all-on-X concept has evolved into a versatile treatment modality, particularly for patients who would prefer not to undergo multiple extensive hard- and soft-tissue augmentation procedures and lengthy, costly tooth-preserving therapies.1 This case report describes the diagnosis, planning and execution of a mandibular full-arch rehabilitation using an entirely digital prosthetic workflow. The case report highlights the clinical rationale behind the treatment plan options and the role of digital tools in achieving a predictable outcome.

Fig. b: Pre-op panoramic radiograph and the findings.
Traditionally, full-arch implant rehabilitation was carried out using conventional impression techniques, requiring multiple appointments and repeated impressions and often causing discomfort for patients. Furthermore, any error during the process usually required starting over with a new impression, and this could be particularly challenging if impression copings had to be removed and repositioned. The advent of intra-oral scanners has introduced a paradigm shift in implant prosthodontics, enabling clinicians to work more efficiently and comfortably while achieving accuracy comparable to that of conventional methods.
Digital workflows have long been implemented in dental laboratories, but their integration into clinical practice in recent years has enabled a seamless transition from digital planning to definitive restoration. Initially, the accuracy of digital impressions for full-arch restorations was debated, and physical impressions were often preferred for large-span rehabilitation. However, the development of advanced scan bodies, particularly horizontal and low-profile designs, has made it possible to achieve highly accurate digital impressions even in full-arch implant cases, in both the maxilla and the mandible. These advancements, along with thoughtful material selection and planning, now allow clinicians to fully leverage the benefits of digital workflows in complex rehabilitation.
Case presentation
A 65-year-old female patient presented with complaints of tooth sensitivity under her existing mandibular prothesis and expressed concern over her missing teeth and periodontal health. The patient also inquired about the feasibility of implants to restore function and aesthetics.
Clinical and radiographic findings
Intra-oral examination revealed compromised mandibular dentition, an old fixed prothesis, missing posterior teeth on the left side, periodontal involvement and gingival inflammation. A panoramic radiograph was obtained, and the findings were reported to the patient (Figs. 1a & b; 2a & b). Both mandibular canines had visible periapical radiolucencies. A CBCT scan was performed for a more detailed assessment of the alveolar bone anatomy (Figs. 3a & b). Temporomandibular joint examination revealed no indication of dysfunction (crepitus, clicking or pain).

Figs. 2a & b: Intra-oral scans of the pre-op situation.

Fig. 2b
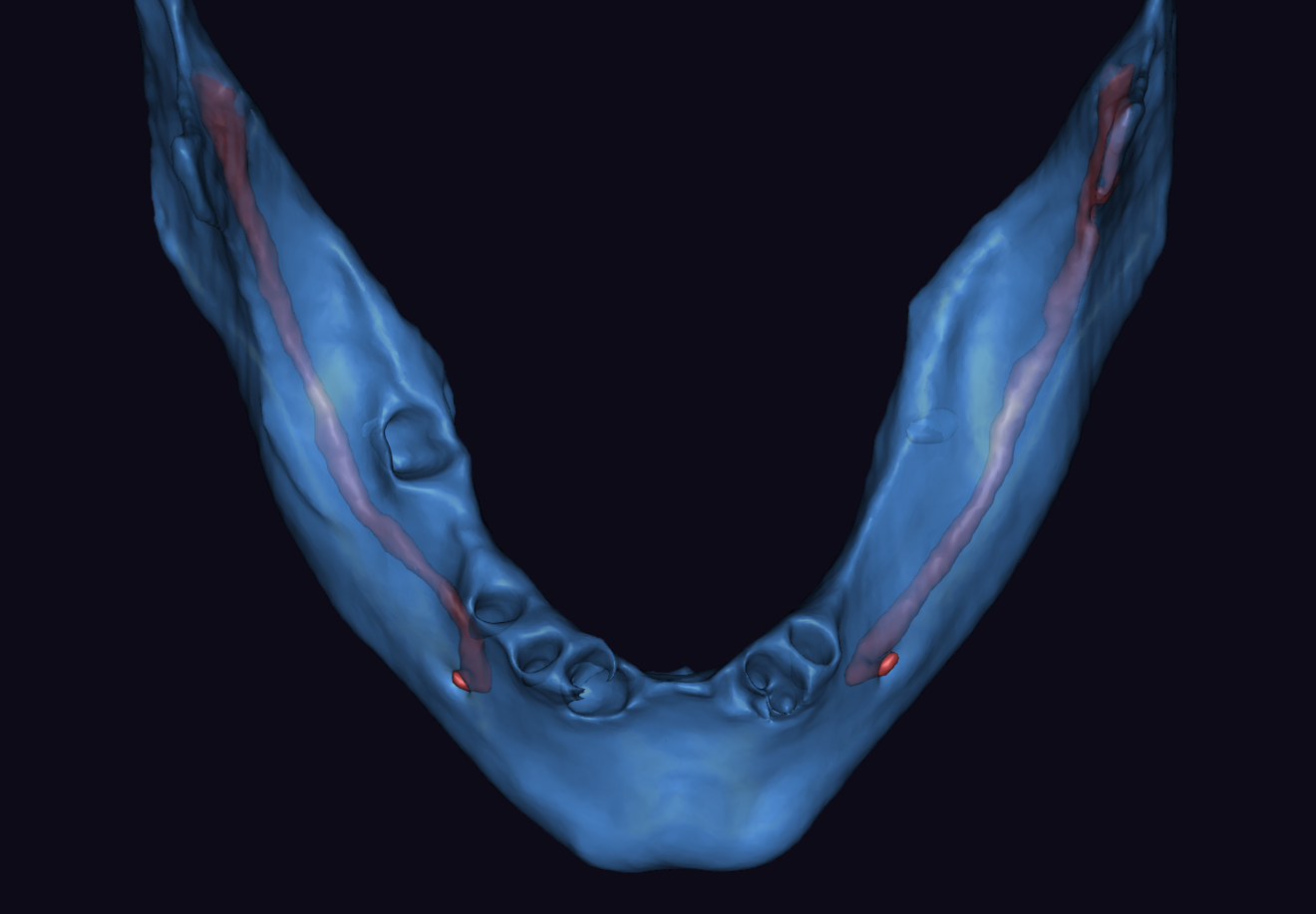
. Mandibular arch morphology after virtual teeth extractions (b).")
Figs. 3a & b: Segmented CBCT scan (a). Mandibular arch morphology after virtual teeth extractions (b).