Immediate placement of implants into fresh extraction sockets has been shown to deliver good outcomes. The literature reports good implant survival rates, as well as acceptable marginal bone loss, gingival recession and aesthetics.1 In particular, there is evidence that immediate implant placement into molar sites leads to predictable outcomes and high success rates.2 The same study suggests that grafting around the implant in these situations and using an anatomic healing abutment can further reduce resorption of the bone.
The following case report demonstrates the successful implementation of immediate implant placement in fresh molar extraction sockets.
Case presentation

Fig. 2: Pre-op radiograph.
A 57-year-old male patient presented by referral with two failing molars, teeth #46 and 47. The patient had a clear medical history, and both molars exhibited extensive caries and restoration (Figs. 1–6).
Treatment planning
After thorough discussion, the patient was presented with two options: deep marginal elevation combined with root canal treatment or implant placement. The patient opted for implants, expressing a preference for a long-term fixed solution.
Given the absence of acute infection and the availability of adequate bone, we decided on immediate implant placement with delayed loading for both sites. Immediate placement is preferred, because maintaining the existing hard- and soft-tissue architecture is far more predictable than attempting to rebuild it later.
A guided surgical approach was selected, specifically a sleeveless guide, to make use of the precision that it affords in such cases. The DentiqGuide software (3DII) was used to plan treatment in order to establish precise implant positioning. The surgical guide was then printed on a Sonic Mini 8K S (Phrozen), ensuring high accuracy in execution.

Fig. 3: Virtual extraction.

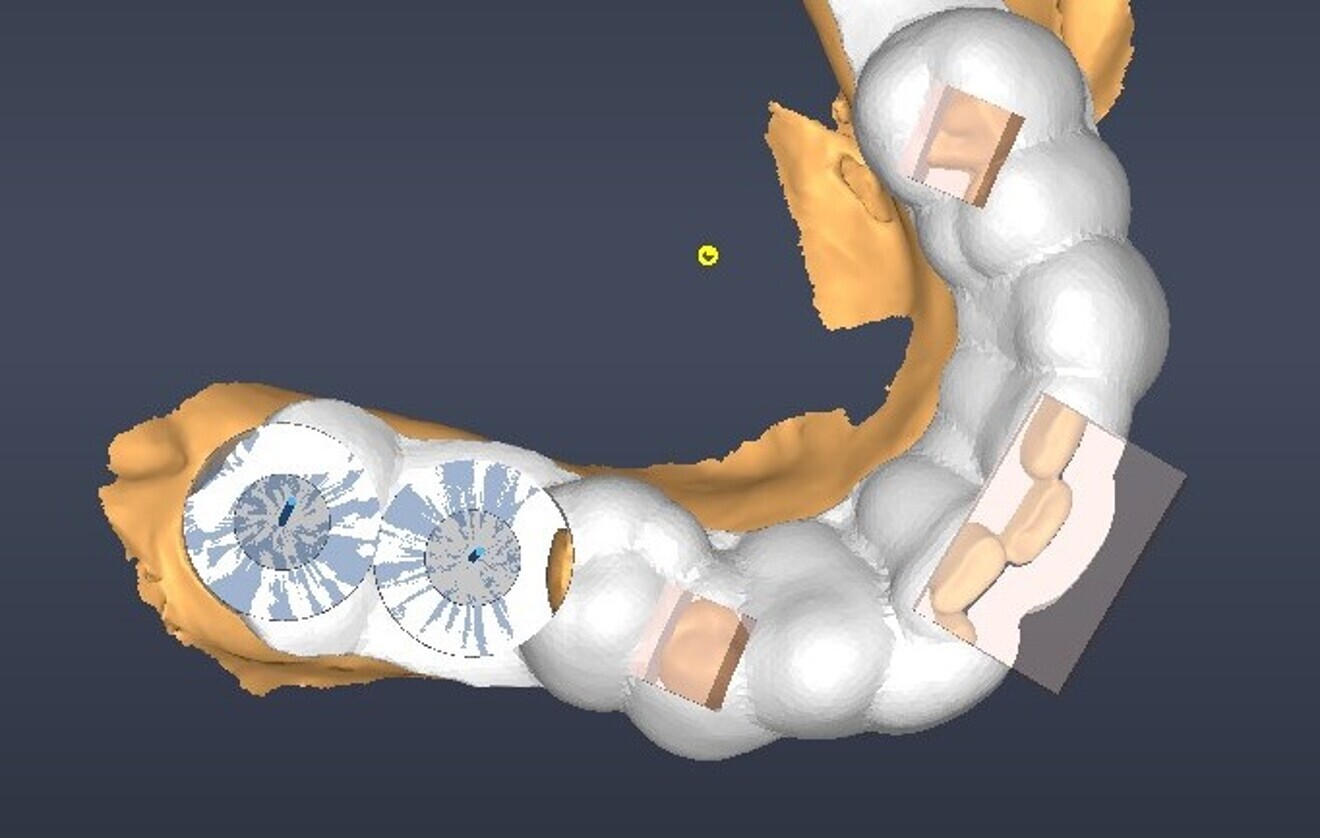
Fig. 4: Digital implant planning, occlusal view.

Fig. 5: Digital implant planning, labial view.