Preconised by Kesling in 1946, treatment with clear aligners was initially used to correct misaligned teeth.1 Currently, aligners dominate the orthodontic market, promising superior advantages over orthodontic treatment with fixed appliances, particularly in terms of aesthetics. 1–3 In addition, there has been significant recent progress in the technological development of computeraided treatment planning and execution.2, 4, 5
Aligner treatment has also been driven by patient demand.1 In Brazil, the pioneering brand (Invisalign, Align Technology) pursued ostentatious marketing in the major television media, leading to great interest among the population. The demand for aligners also gained momentum during the COVID-19 pandemic, during which orthodontic clinical activities ceased owing to lockdown recommendations from the World Health Organization and various countries’ authorities. The need to continue orthodontic treatment led to the use of aligners, owing to the ability of treatment to progress by the patient swapping the aligners. However, after the pandemic period, the need for regular follow-up visits to the orthodontist could be continued for adjustment of the treatment to ensure the best possible result. Failure to plan can result in problems such as delays in treatment, insufficient treatment, misaligned teeth and even permanent damage to the teeth and gingivae.2
 Frontal view. (b) Lateral view. (c) Patient smiling.")
Figs. 1a–c: Orthodontic treatment planning based on extra-oral photographs. (a) Frontal view. (b) Lateral view. (c) Patient smiling.
Adult patients often seek orthodontic treatment, and the incidence of periodontal disease among this group seeking orthodontic treatment is high. Orthodontic treatment using fixed appliances is still the gold standard. It is known that all components of fixed orthodontic appliances (brackets, bands, archwires, etc.), regardless of the technique used, hinder the entire oral hygiene process, favouring the increase of dental biofilm. A significant increase in the count of periodonto-pathogenic microorganisms (Porphyromonas gingivalis, Prevotella intermedia, Prevotella nigrescens, Tannerella forsythia and Fusobacterium species), cariogenic microorganisms (Streptococcus mutans and lactobacilli) and Candida albicans has been reported in patients undergoing fixed orthodontic treatment. The deposition and accumulation of dental biofilm, when not disorganised by mechanical plaque control, by either the patient or the dental professional, leads to the formation of dental calculus, leading to the onset of gingival, periodontal and peri-implant disease.2–7
However, orthodontic treatment for periodontic patients also favours good oral hygiene practices. Resolving diastemas and crowding favours oral hygiene. Besides orthodontic treatment favouring oral health, it addresses patients’ general health.
Adult patients have high aesthetic expectations of orthodontic treatment. From this perspective, it is clear that there must be synergy between the orthodontics and periodontics specialties. Orthodontic management of adult patients with periodontal problems must respect the biology of the patient in terms of time, force and orthodontic pressure. Orthodontic pressure induces an inflammatory process in the periodontium—a predictable response to trauma—but essential in the tooth movement process.4–6
Basically, periodontal disease depends on intrinsic and extrinsic factors, such as host resistance, systemic disease or pathological conditions, smoking, the periodontal phenotype (thickness of bone and gingival tissue), and quantity and microbiological quality of the biofilm, which can interfere with the periodontal disease process. Thus, periodontal control before, during and after orthodontic treatment is essential in order to contribute to periodontal health and better orthodontic management, regardless of the therapy used, including aligners.4,5,7
Because aligners can be removed for oral hygiene, patients may feel that oral hygiene is less of a concern and underestimate its importance. However, adequate oral hygiene is required for satisfactory treatment with aligners. The use of conventional, tufted and interdental brushes, as well as dental floss, prevents the accumulation of dental biofilm, and the initiation and progression of caries and periodontal disease. These oral hygiene procedures should be carried out after eating and before the aligners are repositioned.3,5–7
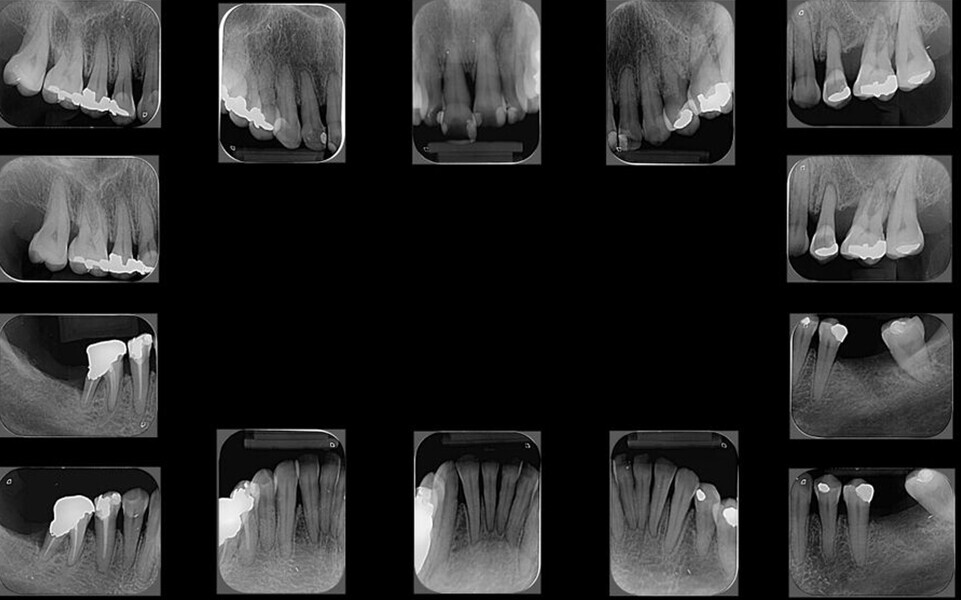
The periodontal treatment of an adult patient undergoing treatment with aligners is illustrated in demonstration of these points. Orthodontic planning considered the extra-oral photographs (Fig. 1) and intra-oral photographs (Figs. 2 & 3). Intra-oral scanning (Fig. 4) and radiographic documentation using panoramic radiographs and cephalometric radiographs (Figs. 5 & 6) were also carried out. From a periodontal perspective, periapical radiographs were recommended (Fig. 7), as this was an adult patient who smoked and showed clinical signs of advanced periodontal disease. Prior periodontal treatment was carried out (Fig. 8) to begin treatment with aligners (Fig. 9).
 Right lateral view. (b) Frontal view. (c) Left lateral view.")
 Maxillary view. (b) Mandibular view.")