Abstract
Objective:
To investigate the efficacy of silver diamine fluoride (SDF) with 5% fluoride varnish (FV) in treating cavitated caries in young children and to explore the association between SDF treatment and oral-health-related quality of life (OHRQoL).
Methods:
Children with active dentinal caries in primary teeth underwent treatment with 38% SDF and 5% FV at baseline and 4 months later. Treated lesions were assessed 4 and 8 months after baseline. Child-level analysis focused on classifying SDF treatment as completely successful if all of a child’s treated lesions were arrested or incompletely successful if at least 1 lesion was not arrested. The Early Childhood Oral Health Impact Scale questionnaire was completed at second and third visits. Statistical analyses included descriptive and bivariate methods. A p value ≤ 0.05 was considered significant.
Results:
This pilot study enrolled 40 children with 239 caries lesions; mean age 40.2 ± 14.9 months and 45% male. Lesion arrest rates after 1 and 2 applications of SDF were 74.1% and 96.2%, respectively. Children who reportedly brushed twice daily were more likely to be in the completely successful group compared with those who brushed less (p = 0.006). Those in the completely successful group had a significantly lower mean baseline dmft score than those in the incompletely successful group (p = 0.048). No significant difference in OHRQoL was observed between the 2 groups.
Conclusions:
SDF with 5% FV is an effective approach to the management of early childhood caries; more than 1 application is recommended, along with regular follow up of patients and twice daily brushing. OHRQoL was not found to be affected by the level of success of SDF treatment.
A common oral problem affecting the pediatric population is early childhood caries (ECC), which is defined as the presence of 1 or more decayed, missing, or filled primary teeth in children < 6 years of age.1 ECC poses treatment challenges for very young children, who are unable to cooperate in the delivery of conventional dental treatment in community-based clinical settings.2 Consequently, many children with ECC must be treated under general anesthesia. Manitoba has some of the highest rates of day surgery to treat ECC in Canada, especially in certain northern and inner-city communities.3,4 Unfortunately, although the surgical approach to managing ECC is often needed, it does not address underlying risk factors for caries. In fact, studies have found relapse rates ranging from 22% to 58.5% after treatment for ECC under general anesthesia.5,6 As a result, many children treated for ECC in this manner require repeat general anesthesia, an undesirable outcome given the risks and costs associated with this treatment modality.7
Silver diamine fluoride (SDF) represents a minimally invasive approach to the management of ECC as an alternative to surgical intervention.8 Although SDF has been successfully used in other countries for decades, it was not approved for use in Canada until 2017.9,10 To the best of our knowledge, there are no published studies investigating the use of SDF in the Canadian population, particularly in toddlers and preschool children. Although several systematic reviews support the efficacy of SDF, they all indicate that further research and clinical trials are needed to establish protocols for optimal case selection and its use.11-14
To our knowledge, only 1 other study has investigated the relation between oral-health-related quality of life (OHRQoL) and SDF treatment of ECC.15 This is an important concept to explore, as it may provide valuable insight into how children and parents perceive the effects of this treatment and how it might affect children’s OHRQoL. In addition, such insight may aid in clinical decision-making regarding which patients may benefit from SDF treatment and which patients may be more appropriately managed with conventional surgical treatment.
The aim of our study was twofold: to investigate the feasibility and efficacy of SDF in treating cavitated caries in young children and to explore the association between SDF treatment and OHRQoL.
Methods
This study was a prospective pilot feasibility trial based on a convenience sample. Ethics approval was obtained from the University of Manitoba’s Biomedical Research Ethics Board. Children were recruited from 3 community clinics in Winnipeg, Manitoba, and the study was conducted between June 2017 and November 2018.
Cooperative children < 72 months of age with at least 1 carious primary tooth meeting International Caries Detection and Assessment System (ICDAS) 5 or 6 criteria (i.e., dentinal caries) and without symptoms of pulpal involvement were included. Children allergic to silver or with hereditary dental alterations of teeth were excluded, as were children with severe medical problems or emergent dental needs.
After providing written informed consent, the child’s caregiver completed a baseline questionnaire, via interview, pertaining to child and family demographics, oral hygiene routines, fluoride intake, dietary habits, dental history and appearance of the teeth. Participants underwent a dental examination without radiographs. Eligible cavitated lesions that were accessible were treated with 38% SDF (Advantage Arrest, Oral Science, Brossard, QC, Canada). No caries excavation was performed; however, gross debris was removed. Using cotton isolation, lesions were dried with air or gauze, and a microbrush was used to apply SDF for up to 1 minute, depending on the child’s cooperation. Treated lesions were then rinsed with water or wiped with wet gauze, followed by FV application (NUPRO 5% NaF white varnish, Dentsply Sirona Canada, Woodbridge, ON, Canada). Parents were instructed to have their child avoid eating and drinking for 30 minutes after application and to refrain from brushing teeth until the next morning (because of the fluoride varnish application, which was used for overall caries prevention).
Four months after the baseline visit, participants returned for a second visit during which treated lesions were assessed to determine caries arrest. Lesions that were hard to tactile probing and black in colour were determined to be successfully arrested. A second application of 38% SDF with 5% FV was performed on all previously treated lesions. Parents were asked to complete an Early Childhood Oral Health Impact Scale (ECOHIS) questionnaire. Approximately 4 months after this second visit, participants returned for a third and final visit for assessment of caries arrest and to complete a follow-up questionnaire and a second ECOHIS questionnaire.
The colour (yellow, brown, black) and hardness (very soft, medium, very hard) of treated lesions as well as the dmft score were recorded at baseline and at each follow-up visit. Hardness was assessed by applying light force to the caries lesion with a probe. A single experienced examiner (RJS) was involved throughout the study and was responsible for the application of SDF as well as the assessment of caries arrest. Child level analysis focused on classifying SDF treatment as completely successful if all treated lesions were found to be arrested and incompletely successful if at least 1 lesion was found not to have been arrested. Treated teeth were assessed for the presence of pain and/or infection at each follow-up visit. The behaviour of the child and difficulty encountered in providing treatment was also documented.
The ECOHIS, which was administered by interview, is a validated questionnaire which uses caregiver responses to assess OHRQoL in preschool children and their families.16 ECOHIS consists of 13 questions divided into 2 sections: the child impact section (CIS) which has 4 domains (symptoms, function, psychological, self-image/social interaction) and the family impact section (FIS) which has 2 domains (parent distress, family function)sup Responses were coded according to ECOHIS protocol: 0 = never, 1 = hardly ever, 2 = occasionally, 3 = often, 4 = very often, 5 = don’t know.16 Total scores were calculated as a simple sum of the responses.16 The CIS score can range from 0 to 36 and the FIS from 0 to 16, with the total possible score ranging from 0 to 52.16 A higher score indicates a greater impact and a poorer OHRQoL.
Data from the clinical assessments as well as from the ECOHIS questionnaires were entered into an Excel (Microsoft, Redmond, Wash., USA) database. Statistical analyses were performed using the Number Cruncher Statistical Software Version 12 (Kaysville, Utah, USA). Both descriptive (frequencies and means) and bivariate (t tests, and Fisher’s exact tests) analyses were performed. A p value ≤ 0.05 was significant.
Results
Participant Characteristics
A total of 40 children (45% male) with a mean age of 40.2 ± 14.9 months were recruited (Table 1). Approximately a third identified as refugees or newcomers (defined as < 2 years in Canada). The mean number of ICDAS 5 and 6 lesions treated per child was 6.0 ± 3.8.
|
Characteristic |
No. (%), except where indicated |
|---|---|
|
Note: dmft = decayed, missing, filled teeth, ICDAS = International Caries Detection and Assessment System, SD = standard deviation. |
|
| Sex
Male Female |
|
| Mean age, months ± SD, range | 40.2 ± 14.9, 17–71 |
| Dental Insurance
Yes No Unsure |
|
| Refugee/newcomer
Yes No |
|
| Ethnicity
African Asian Caucasian Other |
|
| Use of fluoridated toothpaste
Yes No Unsure |
|
| Frequency of tooth brushing
Once daily Twice daily Every other day Never |
|
| Baseline dmft, mean ± SD | 5.9 ± 3.2 |
| No. lesions treated per child (ICDAS 5 and 6), mean ± SD | 6.0 ± 3.8 |
Lesion-Level Analysis
At the baseline visit, 239 caries lesions (111 anterior, 128 posterior) were treated with SDF. The treated lesions were located on primary incisors (40.2%), canines (6.3%), first molars (30.5%) and second molars (23.0%). All participants returned for the second visit. It was determined that 74.1% lesions had arrested after 1 application of SDF (Fig. 1). Two children presented with an abscessed SDF-treated tooth and 1 child had an abscessed tooth extracted before the second visit. The mean dmft score increased from 5.9 ± 3.2 at baseline to 6.0 ± 3.3. The mean time elapsed between baseline and the second visit was 16.7 ± 2.8 weeks.
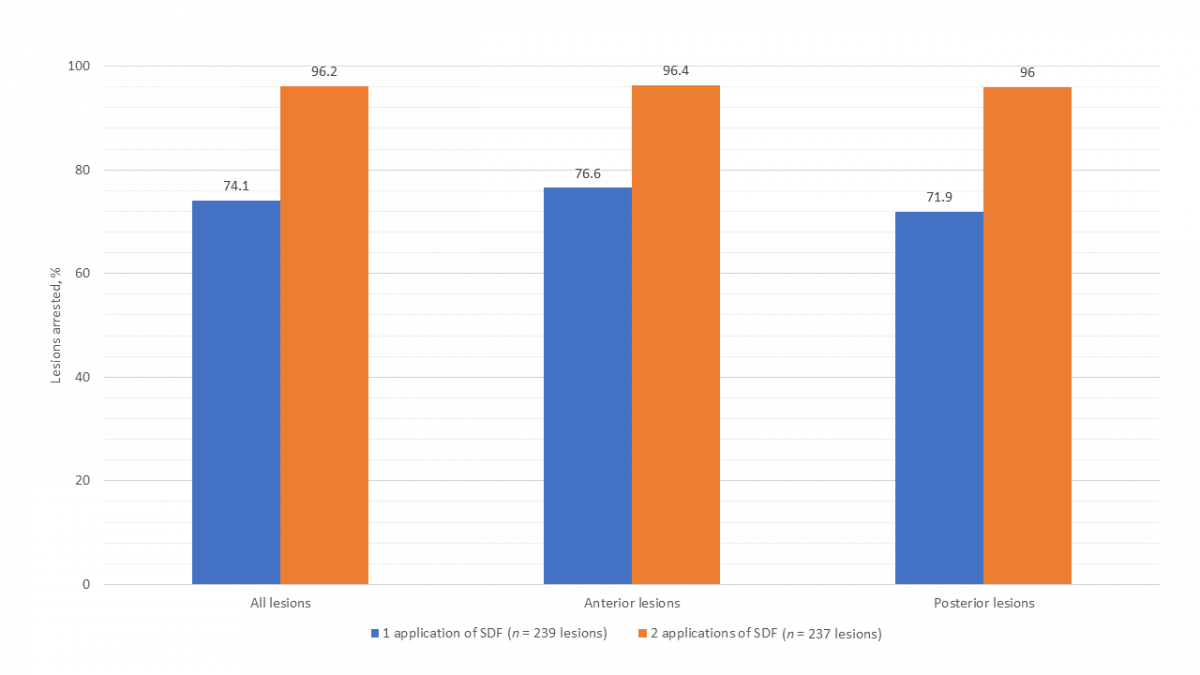
All participants returned for the third and final visit. Two lesions were excluded from analysis as 1 tooth was extracted for an unknown reason before the third visit and another had insufficient data recorded to determine arrest, reducing total lesions to 237 (111 anterior, 126 posterior). It was determined that 96.2% lesions had arrested after 2 applications of SDF (Fig. 1). The mean dmft score increased significantly from 6.0 ± 3.3 at second visit to 6.3 ± 3.3 (paired t test, p = 0.036). The mean time elapsed between the second and third visit was 18.0 ± 3.6 weeks.
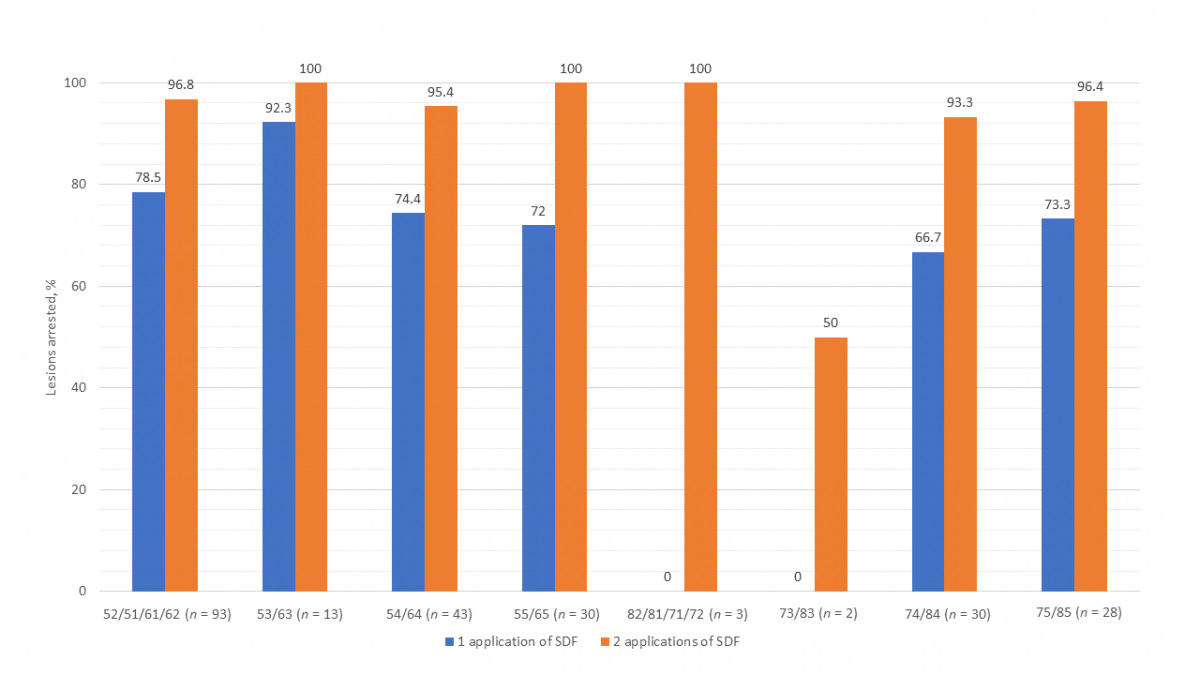
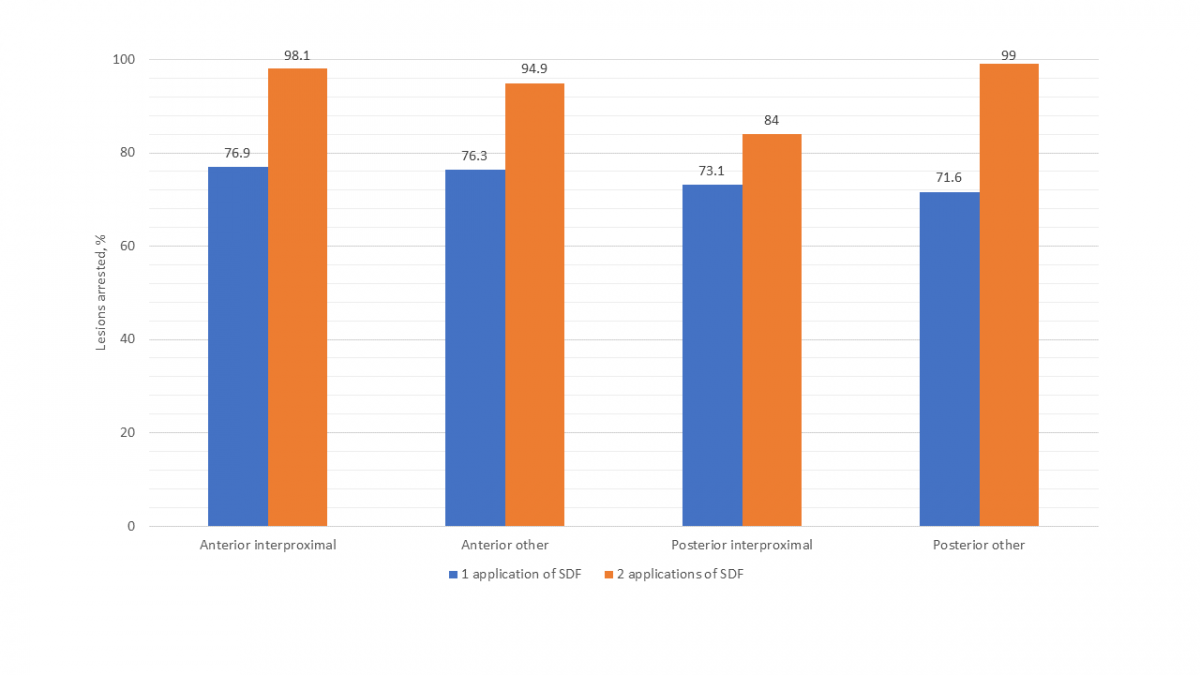
Figure 2 presents the success of SDF by specific primary teeth. Other than the mandibular incisors and canines, which had only 5 lesions, the mandibular first molar had the lowest arrest rate (66.7%) of all teeth after 1 application of SDF. Arrest rates for all teeth were higher after 2 applications of SDF. Although the success of SDF in arresting interproximal lesions versus those on other surfaces was comparable after a single application, after 2 applications, interproximal lesions on posterior teeth were found to have a notably lower arrest rate (Fig. 3).
Child-Level Analysis
At the second visit, 17 (42.5%) participants were determined to be in the completely successful arrest group and 23 (57.5%) in the incompletely successful arrest group. Participants noted above who presented with abscessed teeth following SDF application or for whom arrest data were unknown or missing were classified as incompletely successful. χ2 analyses revealed no significant relation between arrest and sex, frequency of tooth brushing, difficulty providing treatment or use of fluoridated toothpaste (Table 2).
|
Second visit (n = 40) |
Third visit (n = 40) |
|||||
|---|---|---|---|---|---|---|
|
Complete success, no. (%) |
Incomplete success, no. (%) |
p |
Complete success, no. (%) |
Incomplete success, no. (%) |
p |
|
| Sex
Male Female |
|
|
|
|
|
|
| Frequency of tooth brushing
Twice daily < twice daily |
|
|
|
|
|
|
| Difficulty providing treatment
Yes No |
|
|
|
|
|
|
| Use of fluoridated toothpaste
Yes No/unsure |
|
|
|
|
|
|
At the third visit, 34 (85.0%) participants were determined to be in the completely successful arrest group and 6 (15.0%) were found to be in the incompletely successful group. χ2 analysis revealed a significant relation between the frequency of tooth brushing and successful arrest, with brushing twice daily associated with a greater likelihood of being in the completely successful arrest group (p = 0.006). A significant association was observed between baseline dmft score and arrest at third visit, with participants in the completely successful arrest group having a lower mean score of 5.4 compared with 8.8 in the incompletely successful arrest group (2-sample t test, p = 0.048).
ECOHIS
At the second visit, mean total ECOHIS score was 3.8 ± 4.4 out of a possible 52, with mean CIS score 1.9 ± 3.1 out of a possible 36 and mean FIS score 1.9 ± 2.1 out of a possible 16 (Table 3). Third-visit mean scores were 2.7 ± 3.8, 1.3 ± 2.8 and 1.4 ± 2.0, respectively, and were not significantly different from second-visit scores. Only 2 parameters had an increased score: “difficulty drinking” in the CIS and “felt guilty” in the FIS. There was no significant difference in mean total, CIS or FIS scores between completely and incompletely successful groups.
|
Child impact section |
Mean (SD) |
Never, no. (%) |
Hardly ever, no. (%) |
Occasionally, no. (%) |
Often, no. (%) |
Very often, no. (%) |
|---|---|---|---|---|---|---|
| Child symptoms |
0.60 (0.87) |
|||||
| 1. Oral/dental pain |
25 (62.5) |
7 (17.5) |
7 (17.5) |
1 (2.5) |
0 (0) |
|
| Child functions |
0.78 (1.73) |
|||||
| 2. Difficulty drinking |
37 (92.5) |
1 (2.5) |
1 (2.5) |
1 (2.5) |
0 (0) |
|
| 3. Difficulty eating |
35 (87.5) |
2 (5.0) |
1 (2.5) |
1 (2.5) |
1 (2.5) |
|
| 4. Difficulty pronouncing words |
35 (87.5) |
2 (5.0) |
0 (0) |
3 (7.5) |
0 (0) |
|
| 5. Missed preschool or school |
37 (92.5) |
3 (7.5) |
0 (0) |
0 (0) |
0 (0) |
|
| Child psychological factors |
0.33 (0.76) |
|||||
| 6. Trouble sleeping |
37 (92.5) |
2 (5.0) |
1 (2.5) |
0 (0) |
0 (0) |
|
| 7. Irritable or frustrated |
35 (87.5) |
2 (5.0) |
2 (5.0) |
1 (2.5) |
0 (0) |
|
| Child self image/social interaction |
0.23 (0.70) |
|||||
| 8. Avoid smiling or laughing |
36 (90.0) |
2 (5.0) |
2 (5.0) |
0 (0) |
0 (0) |
|
| 9. Avoid talking |
38 (95.0) |
1 (2.5) |
1 (2.5) |
0 (0) |
0 (0) |
|
| Total |
1.93 (3.13) |
|||||
| Family impact section | ||||||
| Parental distress |
1.03 (1.69) |
|||||
| 10. Been upset |
29 (72.5) |
3 (7.5) |
6 (15.0) |
1 (2.5) |
1 (2.5) |
|
| 11. Felt guilty |
31 (77.5) |
1 (2.5) |
6 (15.0) |
2 (5.0) |
0 (0) |
|
| Family function |
0.83 (1.30) |
<...

| ||||