Abstract
Introduction: Establishing dental homes for children at an early age is an important step toward instilling good oral health practices and changing trajectories of oral health. The purpose of this study was to determine how accredited dental and dental hygiene programs in Canada prepare students in the areas of infant, toddler and prenatal oral health.
Methods: An electronic questionnaire was sent to associate deans (academic), program directors or curriculum directors of accredited dental (n = 10) and dental hygiene (n = 39) programs. Participants were asked about infant, toddler and prenatal oral health curricula taught at their institution. Descriptive statistics and bivariate analyses were used to assess the results. A p value ≤ 0.05 was considered significant.
Results: Representatives of 10 dental (100%) and 25 dental hygiene (64.1%) programs responded. All dental and 56% of dental hygiene programs recommend a first visit by 12 months. Infant and toddler oral health was noted as a component of most schools’ curriculum. Barriers to teaching about or providing clinical experiences in infant and toddler oral health include lack of time, patients, program resources and finances. Most dental (70%) and dental hygiene (82.6%) programs include prenatal oral health as a component of their curriculum, yet only 40% of responding dental and 70% of dental hygiene programs reported having designated time in their curriculum for it. Barriers preventing programs from teaching or providing clinical experiences regarding prenatal oral health include lack of time and patients.
Conclusions: Many, but not all dental professional programs are teaching their students about the recommended age for a first dental visit. Better adherence to national guidelines will require programs to address current barriers impeding learning about this important topic and to provide creative opportunities for students regarding prenatal and infant and toddler oral health.
The concept of a dental visit by 12 months of age was first proposed by the American Academy of Pediatric Dentistry in 1986.1 Today, professional organizations recommend a first visit coinciding with the eruption of the first tooth or no later than 12 months of age.2-4 The rationale is based primarily on the argument that such a visit establishes a preventive and cost-effective practice for the caregiver and provides long-term benefits for the child.5
Although the Canadian Dental Association (CDA) first endorsed the visit at 12 months in 2001,1 many practitioners and parents remain uninformed.6,7 The CDA recently announced that improving access to first dental visits is a priority approach to address oral health disparities facing young children.
Early preventive visits, particularly for families at high risk, can help reduce the number of children developing caries and promote preventive care.8-10 However, one of the challenges regarding access to care is the limited number of dentists willing to see infants (≤ 12 months) and toddlers (1–3 years).6,11 A recent survey revealed that some general dentists are willing to see low-risk infants and toddlers, but not those with obvious dental disease.12 Parents who attempt to obtain an early consultation for their child may become discouraged, as some practitioners refuse to see any children under 3 years of age.13
Although many early childhood oral health care advocates suggest an interprofessional approach, we must first understand whether this concept and practice are being taught in undergraduate oral health curricula in Canada. Given the important link between a mother’s oral health and that of her child, further understanding of what is taught about prenatal oral health is essential. Without an engaged dental workforce united on this topic, our medical colleagues will continue to become increasingly frustrated by the lack of dental homes for their pediatric patients.12-14
The Commission on Dental Accreditation of Canada (CDAC) establishes requirements for accreditation to ensure that graduates are capable of addressing the oral care needs of the Canadian public. A search of the CDAC accreditation requirements for a graduating dental student found none specifically addressing infant oral health. Section 2.3.12 of the accreditation requirements for Doctor of Dental Surgery or Doctor of Dental Medicine programs states, “Graduates must be competent in the management of the oral health care of the child, adolescent, adult and geriatric patient.”15 The document does not identify management of infant oral health as a separate requirement, although its inclusion is implied. Similarly, there is no mention of specific requirements relating to infant oral health for a graduating dental hygiene student; these graduates must be “competent to manage health promotion and oral health care for a range of clients within the life cycle, including children, adolescents, adults, and seniors.”16 Because dental development and progression of dental disease during childhood vary greatly from birth to adolescence, the lack of specific inclusion of the infant and toddler age groups may lead to their omission from curricula.
The purpose of this study was to determine the extent to which accredited dental and dental hygiene programs in Canada prepare future clinicians in the areas of infant, toddler and prenatal oral health.
Methods
The study population included an associate dean (academic), program director, chair of pediatric dentistry or curriculum director of the 10 accredited dentistry and 39 dental hygiene programs in Canada. Names of all eligible accredited programs were obtained from the CDAC.17 The University of Manitoba’s Health Research Ethics Board approved this study.
In June 2012, a questionnaire was sent via Survey Monkey to our identified contact at each institution (n = 49). Completing the online questionnaire constituted informed consent. For French-speaking educators, a professionally translated French version of the questionnaire was sent. Reminders along with a questionnaire link were sent to all non-responders monthly; the final reminder was sent in February 2013.
The questionnaire was developed by the project team to collect information on whether, and to what extent, programs were educating students in infant, toddler and prenatal oral health. Specifics explored methods used, hours dedicated to each method and materials used to educate students.
Information was exported to an Excel (Microsoft Corp., Redmond, Wash., USA) spreadsheet and analyzed using NCSS v. 8 (NCSS LLC, Kaysville, Utah, USA). Descriptive statistics (frequencies, means and standard deviations [SD]) and t-tests were conducted with Bonferroni correction as required. A p value ≤ 0.05 was considered significant.
Results
Description of Participants
Representatives of 10 dental (100%) and 25 dental hygiene programs (64.1%) responded. Most (69.6%) of the dental hygiene programs were college based, while the remainder were university based (17.4%) or private (13.0%).
Infant and Toddler Oral Health Curriculum
According to respondents, all 10 dental schools recommend that a child’s first dental visit take place by 12 months of age. However, only 56% of dental hygiene programs recommend visits by this milestone. Most respondents (90% dentistry, 84% dental hygiene) indicated that infant and toddler oral health is an explicit component of their school’s curriculum (Table 1). All respondents indicated that time is designated in their curriculum for this topic. Time devoted to didactic instruction varies; dentistry programs: 6.9 ± 5.7 h (mean ± SD), range 2–20 h; dental hygiene programs: 5.5 ± 2.8 h, range 1–10 h, but the difference between these programs is not significant (p = 0.46).
| Question | Dentistry, no. (%) |
Dental hygiene, no. (%) |
|---|---|---|
| *Note that 2 dental hygiene program respondents did not answer all questions. | ||
| In your school’s curriculum, what age is recommended for a child’s first dental visit? | ||
| 6 months | 0 (0) | 5 (20) |
| By 12 months of age or the 1st birthday | 10 (100) | 9 (36) |
| By 24 months of age or the 2nd birthday | 0 (0) | 6 (24) |
| By 36 months of age or the 3rd birthday | 0 (0) | 2 (8) |
| > 36 months of age or after the 3rd birthday | 0 (0) | 3 (12) |
| Are infant and toddler oral health explicitly noted as a component of your school’s curriculum? | ||
| Yes | 9 (90) | 21 (84) |
| No | 1 (10) | 4 (16) |
| Are infant and toddler oral health explicitly noted as a component of your school’s core competencies? | ||
| Yes | 4 (40) | 14 (56) |
| No | 6 (60) | 11 (44) |
| Do you have designated time in your school’s curriculum for teaching infant and toddler oral health? | ||
| Yes | 10 (100) | 25 (100) |
| No | 0 (0) | 0 (0) |
| Does your school offer additional elective training in infant and toddler oral health education? | ||
| Yes | 4 (40) | 1 (4.4) |
| No | 6 (60) | 22 (95.6) |
| Amount of time devoted to infant and toddler oral health in your school’s total didactic curriculum, h (mean ± standard deviation) | 6.9 ± 5.7 | 5.5 ± 2.8 |
Few programs offer additional elective training. Only 1 dental hygiene (4.4%) and 4 dentistry schools (40%) reported offering such opportunities. Such training most commonly takes place in community programs, public health clinics and pediatric dentistry clinics, with considerable variation in hours of exposure (11.8 ± 12.3 h, range 3–30 h).
In terms of the time devoted to various teaching methods, lectures and seminars were the most common didactic approaches followed by clinical care and clinical observation only (Table 2). There were no apparent differences between dental and dental hygiene programs in amount of teaching time. Although dental hygiene respondents reported more hours devoted to didactic instruction, Bonferroni correction revealed that the difference was not significant.
| Teaching method | Dentistry, h (mean ± SD; range) |
Dental hygiene, h (mean ± SD; range) | p* |
|---|---|---|---|
| *Bonferroni correction to address inflated type I error. Significance then set at p ≤ 0.008; hence, no comparisons are statistically significant. | |||
| Lectures and seminars | 3.0 ± 0.67 (2–4) |
4.6 ± 2.6 (1–12) |
0.01 |
| Video, Internet or web-based learning | 0.4 ± 0.97 (0–3) |
0.7 ± 0.97 (0–3) |
0.43 |
| Clinical (observation only) | 2.2 ± 3.1 (0–10) |
1.3 ± 3.1 (0–10) |
0.45 |
| Clinical dental screening | 0.7 ± 1.1 (0–3) |
1.7 ± 3.3 (0–12) |
0.19 |
| Clinical patient care (prevention and/or restorative) | 2.5 ± 2.8 (0–9) |
3.5 ± 4.4 (0–12) |
0.52 |
| Other teaching methods | 0.3 ± 0.9 (0–3) |
0.7 ± 2.2 (0–10) |
0.48 |
Less than a third of dental and dental hygiene programs reported that all students receive clinical hands-on experience in performing infant and toddler examinations (Table 3). Most responding dental (60.0%) and dental hygiene programs (52.2%) rely on their institution’s clinic to provide these opportunities, while others send students to primary care clinics, daycares and public health settings. Of those who provide hands-on examination experiences to some or all of their students, most dental programs (5/9) reported that fewer than 50% of their students receive 1 or more clinical hands-on experiences while most dental hygiene programs (8/14) reported that ≥ 75% of their students have such opportunities (Table 3).
| Question | Dentistry, no. (%) |
Dental hygiene, no. (%) |
|---|---|---|
| *Note that 2 dental hygiene program respondents did not answer all questions. | ||
| Clinical experience | ||
| Clinical hands-on experience: infant/toddler oral health examinations | ||
| All students have experience | 3 (30) | 7 (30.4) |
| Variable experience for students | 6 (60) | 7 (30.4) |
| No experience for students | 1 (10) | 9 (39.1) |
| One or more infant/toddler clinical hands-on experiences | ||
| < 5% | 0 (0.0) | 2 (14.3) |
| 5–10% | 3 (33) | 1 (7.1) |
| 25–49% | 2 (22) | 0 (0.0) |
| 50–74% | 1 (11) | 3 (21.4) |
| 75–100% | 3 (33) | 8 (57.1) |
| Collaboration to expose students to infants/toddlers (all that apply) | ||
| Primary care clinics | 3 (30) | 5 (20) |
| Community dental clinics | 5 (50) | 4 (16) |
| Public health settings or programs | 2 (20) | 15 (60) |
| Pediatric dentists (private practice) | 1 (10) | 3 (12) |
| Daycares | 1 (10) | 14 (56) |
| Other (please specify): | 3 (30) | 2 (8) |
| Didactic experience | ||
| Amount of toothpaste | ||
| Yes | 10 (100) | 23 (100) |
| No | 0 (0) | 0 (0) |
| Unsure | 0 (0) | 0 (0) |
| Benefits and frequency of fluoride varnish to prevent and arrest caries | ||
| Yes | 10 (100) | 20 (87.0) |
| No | 0 (0) | 1 (4.4) |
| Unsure | 0 (0) | 2 (8.7) |
| Apply fluoride varnish | ||
| Yes | 9 (90) | 18 (78.3) |
| No | 0 (0) | 4 (17.4) |
| Unsure | 1 (10) | 1 (4.4) |
| Discuss proper diet with caregivers? | ||
| Yes | 9 (90) | 19 (82.6) |
| No | 1 (10) | 2 (8.7) |
| Unsure | 0 (0) | 2 (8.7) |
| Perform and position for an oral health examination | ||
| Yes | 10 (100) | 18 (78.3) |
| No | 0 (0) | 2 (8.7) |
| Unsure | 0 (0) | 3 (13.0) |
| Recognize dental caries | ||
| Yes | 10 (100) | 22 (95.7) |
| No | 0 (0) | 0 (0) |
| Unsure | 0 (0) | 1 (4.4) |
| Curriculum content (professional policies and guidelines included in the infant/toddler curriculum) | ||
| Dental home | ||
| Yes | 10 (100) | 11 (47.8) |
| No | 0 (0) | 5 (21.7) |
| Unsure | 0 (0) | 7 (30.4) |
| Infant oral health care | ||
| Yes | 10 (100) | 19 (82.6) |
| No | 0 (0) | 3 (13.0) |
| Unsure | 0 (0) | 1 (4.4) |
| Definition of early childhood caries | ||
| Yes | 10 (100) | 21 (91.3) |
| No | 0 (0) | 0 (0) |
| Unsure | 0 (0) | 2 (8.7) |
| Caries-risk assessment tools | ||
| Yes | 9 (90) | 22 (95.6) |
| No | 1 (10) | 0 (0) |
| Unsure | 0 (0) | 1 (4.4) |
Many respondents indicated that their programs expose students to working with high-risk infant and toddler populations, e.g., Aboriginal (dentistry 40%, dental hygiene 32%), low-income (80%, 72%), refugees (60%, 20%). Dentistry and dental hygiene programs appear to have limited inter-professional learning opportunities for their students (30%, 47.8%).
Barriers to teaching about or providing clinical experiences in infant and toddler oral health include lack of time, patients, program resources and finances (Fig. 1).
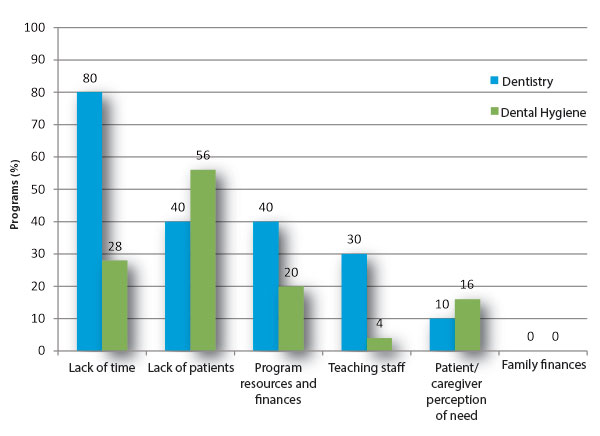 Figure 1: Barriers to teaching or providing clinical experience in infant and toddler oral health in dentistry (n = 10) and dental hygiene (n = 25) programs.
Figure 1: Barriers to teaching or providing clinical experience in infant and toddler oral health in dentistry (n = 10) and dental hygiene (n = 25) programs.
Key policies and clinical guidelines related to infant and toddler oral health appear to be present in curricula (Table 3). Other concepts related to infant oral health, such as the use of fluoride toothpastes and varnishes, infant feeding practices and caries diagnosis, are also taught (Table 3). Most programs recommend fluoridated toothpaste for infants and toddlers (dentistry 80%, dental hygiene 65.2%). Nearly all respondents were aware that their program discusses professional recommendations for a first dental visit (dentistry 100%, dental hygiene 91.3%) and were aware of the CDA’s position statement on early childhood caries2 (dentistry 100%, dental hygiene 82.6%). All respondents reported being aware of the CDA’s position statement on fluoride18 (dentistry 100%, dental hygiene 100%).
All respondents indicated that their curriculum teaches students about the relationship between bottle feeding and oral health, while 90% of dental and 87% of hygiene programs reported teaching students about breastfeeding and oral health.
Prenatal Oral Health Curriculum
Respondents noted that in most dental (70%) and dental hygiene (82.6%) programs, prenatal oral health is a component of the curriculum (Table 4). Time is designated in the curriculum of 40% of dental and 69.6% of hygiene programs for teaching prenatal oral health. Educating students about the relation between periodontal disease during pregnancy and premature birth and low birthweight was commonly reported (dentistry 70%, dental hygiene 95.7%). Most respondents also reported that their program informs students about the role of prenatal nutrition in infant oral health (dentistry 80%, dental hygiene 91.3%). All reported teaching about bacterial transmission from mother to infant.
Details on methods used and time devoted to prenatal oral health appear in Table 5. Barriers to teaching or providing clinical experiences in prenatal oral health include lack of patients and time in the curriculum (Fig. 2).
| Question | Dentistry, no. (%) | Dental hygiene, no. (%) |
|
|---|---|---|---|
| *Note that 2 dental hygiene program respondents did not answer all questions. | |||
| Explicitly noted as a component of your school’s curriculum? | |||
| Yes | 7 (70) | 19 (82.6) | |
| No | 1 (10) | 3 (13.0) | |
| Unsure | 2 (20) | 1 (4.4) | |
| Explicitly noted as a component of your school’s core competencies? | |||
| Yes | 4 (40) | 10 (43.5) | |
| No | 4 (40) | 10 (43.5) | |
| Can be done as an elective | 0 (0) | 1 (4.4) | |
| Unsure | 2 (20) | 2 (8.7) | |
| Designated time in your school’s curriculum (either through your department or other departments)? | |||
| Yes | 4 (40) | 16 (69.6) | |
| No | 2 (20) | 4 (17.4) | |
| Unsure | 4 (40) | 3 (13.0) | |
| Contemplating adding prenatal oral health o curriculum? | |||
| Yes, within the next 12-24 months | 3 (30) | 5 (21.7) | |
| No | 1 (10) | 7 (30.4) | |
| Unsure | 6 (60) | 11 (47.8) | |
| Additional elective training in prenatal oral health education? | |||
| Yes | 0 (0) | 3 (13.0) | |
| No | 7 (70) | 20 (87.0) | |
| Unsure | 3 (30) | 0 (0) | |
| Students who have 1 or more prenatal clinical hands-on experiences, % | |||
| None | 5 (50) | 3 (13.0) | |
| < 5 | 0 (0) | 5 (21.7) | |
| 5–10 | 2 (20) | 3 (13.0) | |
| 11–24 | 0 (0) | 3 (13.0) | |
| 25–49 | 0 (0) | 2 (8.7) | |
| 50–74 | 0 (0) | 2 (8.7) | |
| 75–100 | 0 (0) | 4 (17.4) | |
| Unsure | 3 (30) | 1 (4.4) | |
| Which department(s) or discipline(s)/course(s) is/are responsible for teaching prenatal oral health? (check all that apply) | |||
| Periodontal | 2 (20) | 5 (20) | |
| General dentistry/operative dentistry | 0 (0) | 1 (4) | |
| Public health/community dentistry | 5 (50) | 17 (68) | |
| Pediatric dentistry | 7 (70) | 7 (28) | |
| Unsure | 2 (20) | 3 (12) | |
| Other (please specify): | 0 (0) | 9 (36) | |
| Amount of time in your school’s total curriculum devoted to prenatal oral health, h (mean ± SD) | 2.6 ± 3.8 | 3.5 ± 2.5 | |
| Dentistry, h (mean ± SD; range) | Dental hygiene, h (mean ± SD; range) |
p value | |
|---|---|---|---|
| Lectures and seminars | 2.0 ± 3.1 (0–10) |
2.8 ± 2.3 (0–10) |
0.44 |
| Video, Internet or web-based learning | 0.0 ± 0.0 | 0.4 ± 0.9 (0–4) |
— |
| Clinical (observation only) | 0.0 ± 0.0…

|