
 This month’s prosthodontips is about a common clinical scenario that can very easily catch you out; restoration of a lower second molar.
This month’s prosthodontips is about a common clinical scenario that can very easily catch you out; restoration of a lower second molar.
Access is difficult, isolation is difficult, and the lower second molars are very sensitive to changes in occlusion. For these reasons a simple treatment can quickly become complicated.
Lower second molar case
This week’s patient presented with pain and sensitivity on her LL7. She had been seen by numerous dentists, and provided with a number of composite restorations, and a ceramic onlay. However, no solution was found.
The patient reported that the LL7 initially required a small composite filling.
This never felt right after placement; the tooth became tender to eat on, and sensitive. This composite was removed, and the patient was advised the tooth may be cracked, and an onlay was recommended.
Despite a number of adjustments, the tooth was still symptomatic. This is when the patient presented to me.

The next photos show the patient’s occlusion.
When analysing the occlusion on a symptomatic lower second molar I am assessing for contact in dynamic movements. These will cause hight forces on the tooth. These forces are high as this tooth is close to the TMJ – the forces are highest closest to the joint; similar to a nutcracker.
 Figure 2: ICP. Here you can see the ICP contacts in green. There are fairly even contacts between the LL5, 6 and 7. Molars are well accepting of apical forces in ICP. However, when they are exposed to lateral forces – for example in dynamic occlusal movements, they can become symptomatic
Figure 2: ICP. Here you can see the ICP contacts in green. There are fairly even contacts between the LL5, 6 and 7. Molars are well accepting of apical forces in ICP. However, when they are exposed to lateral forces – for example in dynamic occlusal movements, they can become symptomatic




- 1
- 2
- 3
- 4
- 5
- Previous
- Next
Occlusal issues
In this case I can see a number of issues with the occlusion, and a number of areas to improve upon.
However, at the moment an occlusal cause of pain is only a theory. There are a number of other possibilities – caries, PA pathology, cracked tooth, atypical facial pain.
In order to further diagnose the cause of pain I need to remove the onlay and assess (as the radiograph was inconclusive).
I used the opportunity to prescribe a diagnostic wax up, which was not in contact in dynamic occlusion.

Final result
We fabricated a provisional onlay using the diagnostic wax up. We reviewed the patient four weeks later.
Thankfully all symptoms disappeared. This confirms the diagnosis of pain due to occlusal interferences.
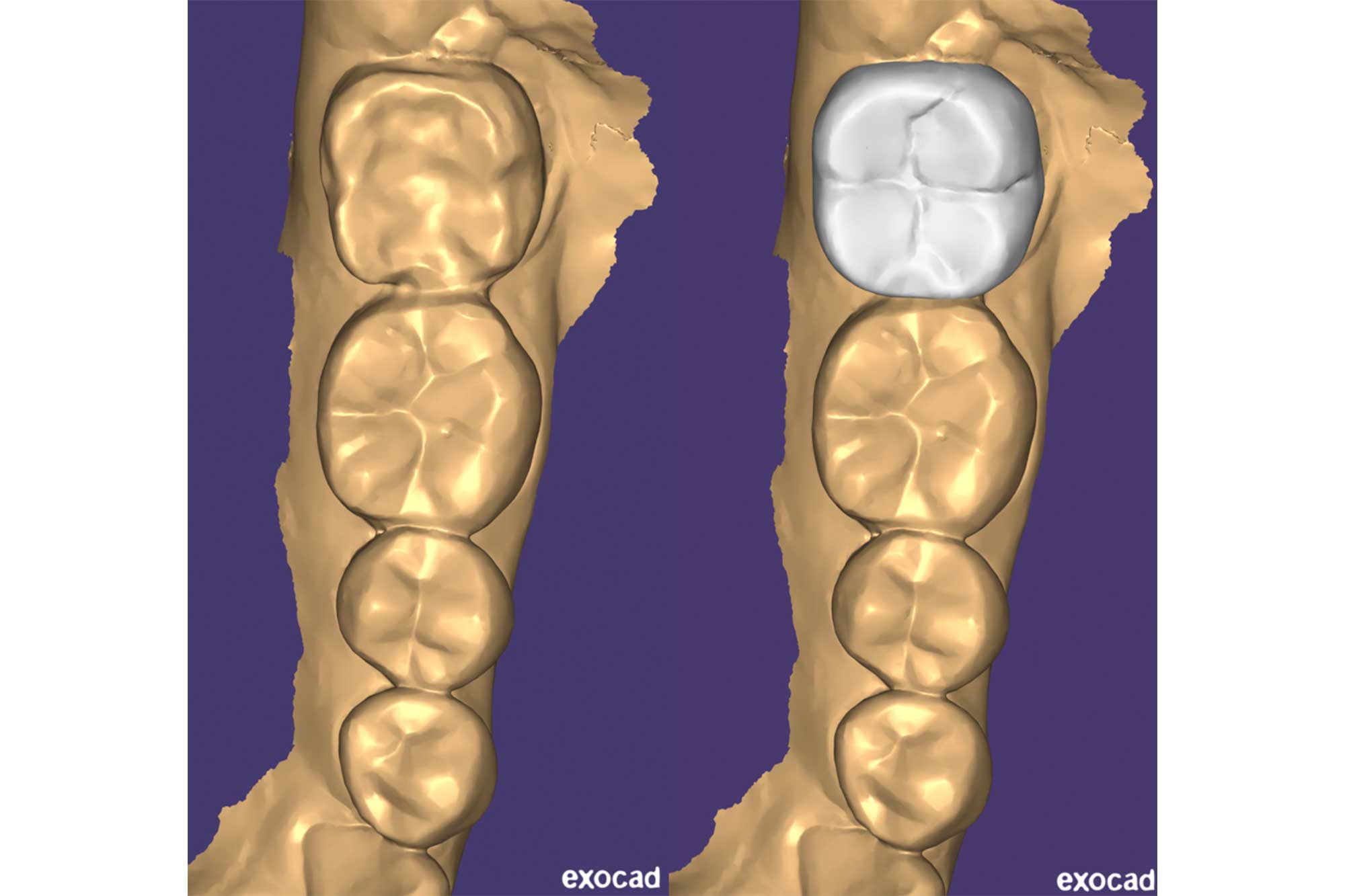
 Figure 9: This shows the definitive onlay – fabricated to match the design of the provisional restoration
Figure 9: This shows the definitive onlay – fabricated to match the design of the provisional restoration


- 1
- 2
- 3
- Previous
- Next
Once we bonded the definitive onlay into place we checked the occlusion. On review the patient remained symptom free.
The takeaway massage from this month’s column – always consider static and dynamic occlusion. Especially in lower second molars!
Please keep the questions coming for the Prosthodontips team. You can contact us on Instagram (@sharplingdental and @prostho_zo) and also email ([email protected]).
If there are specific topics you would like us to cover in a column, please let us know.
Previous Prosthodontips:
- Resin-retained bridges: fun and predictable
- What’s the solution to occlusion confusion?
- Dental ceramics
- Immediate dentures
- Implant salvage.
Follow Dentistry.co.uk on Instagram to keep up with all the latest dental news and trends.