
Abstract
Introduction:
Although condylar fractures are common in the field of oral and maxillofacial surgery, the approach to their treatment is not straightforward. Multiple soft-tissue approaches are available, but it is unclear which yields the best outcomes. In this retrospective study, we aimed to determine whether a transparotid or submandibular soft-tissue approach to treating condylar fractures yields better outcomes.
Methods
This study consisted of a retrospective chart audit and an in-person assessment. The chart audit involved all patients who presented to the Queen Elizabeth II Health Sciences Centre (Halifax) between 2012 and 2022 with condylar fracture treated with open reduction and internal fixation. The chart review assessed each patient’s maximum interincisal opening, paresthesia, nerve function, infection and occlusion. The in-person assessment further assessed scar satisfaction, overall patient satisfaction with the treatment process and cosmetic results, and the incidence of Frey syndrome. Outcomes with the transparotid and submandibular approaches were compared using the Mann–Whitney U test for continuous variables and the χ2 or Fisher exact test for categorical variables, with significance level set at p < 0.05 (2-tailed).
Results:
Data were collected from the charts of 32 patients who met the eligibility criteria during the study period; 14 of these patients also underwent an in-person assessment (at 1 to 7 years after the surgery). Statistical analysis of data from the chart audit and in-person assessment suggested no difference between the 2 approaches in terms of surgical outcomes after condylar fractures.
Conclusions:
The optimal approach for treatment of condylar fractures should be determined individually, based on the surgeon’s preference, fracture location and extent of the fracture.
Introduction
Oral and maxillofacial surgeons commonly treat mandibular fractures. Condylar fractures account for roughly 24% of mandibular fractures, presenting as a sole or secondary fracture, depending on the mechanism of injury.1 The mandibular condyle is subdivided into 3 regions: the condylar head, condylar neck and subcondylar region1 (Fig. 1); fractures can occur in any of these areas.
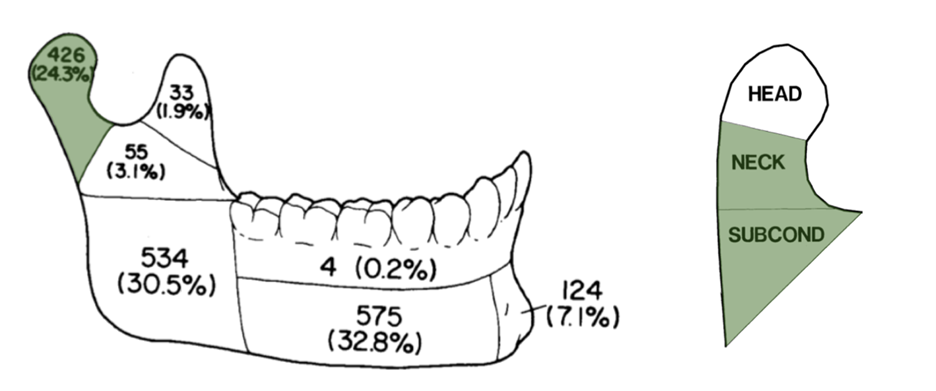
Figure 1: Prevalence of mandibular fractures and regions of the mandibular condyle. HEAD = condylar head; NECK = condylar neck; SUBCOND = subcondylar region.
Fractures can be classified with the Spiessl and Schroll system, where they are categorized by degree of displacement and height of the fracture.2 Type I fractures are nondisplaced or minimally displaced and are typically treated with a closed approach, which involves rigid maxillomandibular fixation to prevent excessive jaw movement and allows the bone to heal indirectly through callus formation. If the fracture is excessively displaced or dislocated (Spiessl and Schroll types II–V), the decision may be made to treat it by open reduction and internal fixation (ORIF). The condylar fractures most commonly treated with ORIF are type II (low fractures with displacement) and type IV (low fractures with dislocation).2 In ORIF, the general concept is that an incision is made to expose the fracture site, the fracture is reduced, and surgical plates are placed to fix the fracture.1,3 In the current study, we focused solely on cases in which ORIF approaches were used to treat condylar fractures.
Multiple ORIF approaches are available to treat condylar fractures; however, the 2 most commonly used at our centre are the transparotid (TP) and submandibular (SM) approaches. The incision for the TP approach is made inferior to the ear lobe and parallel to the posterior border of the ramus.4 The incision for the SM approach is made near the angle of the mandible and parallels the inferior border of the mandibular body4 (Fig. 2a and 2b). Other approaches include the preauricular approach, commonly used in temporomandibular joint surgery, where an incision is made in the natural crease just anterior to the auricle, and the intraoral approach, which is usually reserved for very low subcondylar fractures due to the relatively difficult visualization.
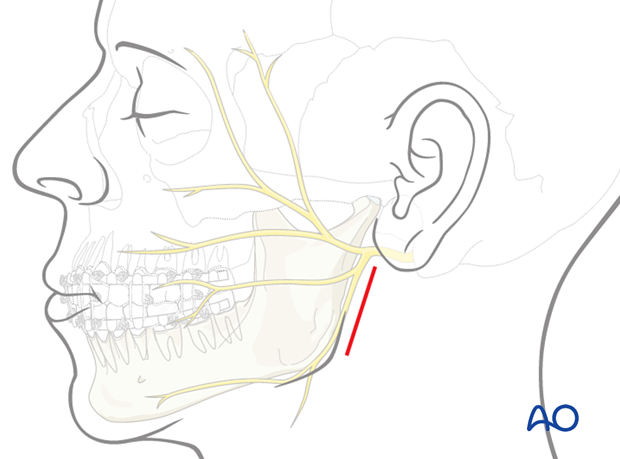
Figure 2a: Schematic of incisions for a transparotid approach. The red line indicates an example fracture site. Adapted, with permission, from AO Foundation. Available: aofoundation.org
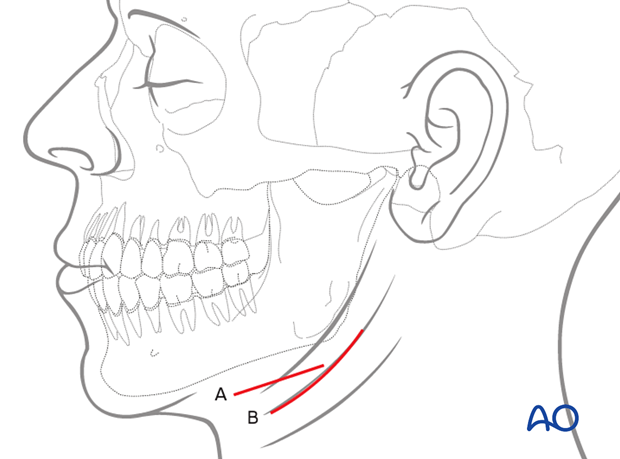
Figure 2b: Schematic of incisions for a submandibular approach. Labels “A” and “B” are different incision designs for a submandibular approach. Adapted, with permission, from AO Foundation. Available: aofoundation.org
The main benefit of a TP approach is proximity to the area of the fracture, which makes plate fixation easier.5,6 A TP approach also facilitates the placement of more than one fixation plate at optimal angles, maximizing stability. However, the smaller incision may make visualization of the fracture more difficult.5,6 The greatest drawback of the TP approach is proximity to the facial nerve trunk, which increases the risk for iatrogenic nerve damage.7 In contrast, although the incision for an SM approach is further from the facial nerve trunk, it is also further from the area of the fracture, making fixation of the plates more difficult.4
It is currently unclear whether the TP or the SM approach yields better surgical results with fewer postoperative complications. In this study, we investigated which of the 2 approaches yields better surgical outcomes, with fewer postoperative complications, with the ultimate goal of determining which can be regarded as the more favourable approach for future surgeries.
Methods
Study Design
Our retrospective cohort study was conducted in 2 parts: a retrospective chart audit and an in-person assessment. Participants were selected from all patients who presented to the Queen Elizabeth II Health Sciences Centre (Halifax) between January 1, 2012, and January 1, 2022, with condylar fracture treated with ORIF. Patients were included if they had a unilateral condylar or subcondylar fracture that was treated by a TP or SM approach. Patients were excluded if they had bilateral fractures, fractures that were not treated with ORIF or fractures that were not treated by a TP or SM approach; patients who were missing at the time of postsurgical follow-up and those who passed away postoperatively were also excluded. All information for the chart audit was collected from the second-week follow-up appointment. This time point was selected because 2 weeks is a required follow-up period (as per department protocol), it allowed for the greatest number of participants, and it was deemed to have allowed for an appropriate amount of initial soft-tissue healing.
All patients in the chart audit group were contacted to participate in an in-person assessment; patients who were unable to attend the in-person assessment were excluded from that portion of the study. Figure 3 outlines the study design and participant selection process in more detail. All in-person participants received compensation, as approved by the institutional research ethics board.
Study protocol and ethics approval was obtained from the Nova Scotia Health (NSH) Research Ethics Board (#1027886), which allowed us to collect nonidentifiable personal health information. Patients who met the inclusion criteria were contacted to obtain their informed consent for a more thorough review of their chart. Patients who consented to participate in the in-person assessment signed an informed consent form at the time of the study, as approved by the NSH Research Ethics Board.
Variables
The predictor variable for this study was treatment of condylar fracture using either a TP or SM approach, as previously defined.
The retrospective chart audit portion of the study explored maximum interincisal opening (MIIO), paresthesia, motor weakness, postoperative infection and changes from preoperative occlusion as outcome variables. The MIIO was defined as the distance from the incisal edge of the most extruded maxillary central incisor to the incisal edge of the most extruded mandibular central incisor when the patient’s mouth was open as wide as was comfortably possible. Paresthesia was defined as loss of normal sensation of the skin overlying areas innervated by the trigeminal nerve and/or the superficial cervical plexus of veins. Motor weakness at 2 weeks after surgery was defined as weakness of the muscles of facial expression that are innervated by the facial nerve. Postoperative infection was defined as the presence of any of the cardinal signs of infection not attributable to motor weakness or the normal swelling expected after surgery. Changes from preoperative occlusion were defined as grade 1, where there was recovery to preinjury occlusion (as stated by the patient), or grade 2, where there was mild malocclusion requiring prosthodontic or orthodontic treatment.
The in-person assessment involved determination of paresthesia, postoperative infection and changes from preoperative occlusion, as defined above, as well as assessment of Frey syndrome, motor weakness, patient and observer scar satisfaction, and overall patient satisfaction. Frey syndrome is a rare neurologic condition in which mastication induces hidrosis and facial flushing because fibres of the glossopharyngeal nerve have been damaged during dissection through the parotid gland.8 The TP approach involves gross dissection through the parotid gland, and Frey syndrome may thus be more prevalent with that approach. Motor weakness at the time of the in-person assessment was defined as reduction or complete loss of function of the muscles of facial expression innervated by the facial nerve and was assessed using the House–Brackmann scale (as outlined in Table 1).9 This scale was selected because it has been considered the benchmark for a simple, validated and reliable test to assess facial nerve damage.10 Patient and observer satisfaction with healing of the scar was based on the Patient and Observer Scar Assessment Scale (POSAS), version 2.0.11 The POSAS is a validated tool that has been used worldwide to assess scarring in surgical patients.11 Finally, overall patient satisfaction was defined as the patients’ satisfaction with the treatment process, including the surgery, postsurgical care and overall results. To date, the literature contains only limited studies with similar outcomes assessing patients’ attitudes toward and satisfaction with the surgery itself.
|
Grade |
Description of weakness |
Measurement of displacement (mm) |
Function (%) |
Estimated function (%) |
|---|---|---|---|---|
| I | Normal | 8/8 | 100 | 100 |
| II | Slight | 7/8 | 76–99 | 80 |
| III | Moderate | 5/8 or 6/8 | 51–75 | 60 |
| IV | Moderately severe | 3/8 or 4/8 | 26–50 | 40 |
| V | Severe | 1/8 or 2/8 | 1–25 | 20 |
| VI | Total | 0/8 | 0 | 0 |
Additional variables assessed in this study (which were used to exclude the possibility of confounding variables) were age, sex, side of the fracture (left or right), location of the fracture (subcondylar or condylar), number of fixation plates used, smoking, alcohol consumption and diabetes. Smoking and alcohol consumption were defined as the use of any amount of the substance(s) at the time of surgery. Diabetes was defined as prior diagnosis of type 1 or type 2 diabetes mellitus with no resolution at the time of the surgery.
Data Collection
To measure MIIO, the patient was asked to open their mouth as wide as possible without assistance. A ruler was then zeroed at the incisal edge of the mandibular central incisors. The measurement was taken at the level of the incisal edge of the maxillary central incisors, with the ruler resting gently on the teeth, without any bends.
Paresthesia was assessed using the cotton wisp test. This involved using a cotton ball and, with the patient’s eyes closed, lightly touching different areas of the face that correspond with the various sensory nerves in the maxillofacial region. The patient was then asked whether they felt anything. To further increase the validity of this test, the patient was also asked if they felt anything without the investigator having touched any area of their face. Paresthesia was documented as being absent or present, depending on whether the patient did or did not feel the cotton wisp, respectively.
As indicated above, motor weakness was assessed using different methods in the 2 parts of the study. For the chart audit portion, motor weakness was assessed as present or absent based on objective findings during the 2-week follow up appointment. This assessment would have involved asking the participant to perform a variety of movements involving the muscles of facial expression. For the in-person assessment portion of the study, the House–Brackmann scale was used to assess weakness of the facial nerve.9 This method involves placing a measurement device with 1-mm markings at the labial commissures and the upper eyelid on each side of the face and asking the participant to smile and lift their eyebrows, respectively. Total displacement is measured for both the mouth and the eye and is evaluated over a maximum total of 8 mm. A score of 8/8 indicates a normal nerve with 100% function.
In the chart audit portion of the study, infection was defined as the presence of any of the cardinal signs of infection (redness, warmth, swelling, pain, loss of function) that were not attributable to motor weakness. Swelling after surgery is normal because of increased postoperative vascularity in the area. If swelling persisted or worsened, and was associated with increased pain and redness, it was considered an infective process. During the in-person assessment, participants were asked if they had experienced any of the cardinal signs of infection after their follow-up appointments, and their responses were cross-referenced with the postoperative chart notes.
Given that participants would likely have presented to the hospital with a malocclusion due to their injury, the preoperative and postoperative chart notes, as well as participants’ descriptions of their teeth before injury, were reviewed to ensure the accuracy of our findings.
Frey syndrome was assessed by asking patients whether they experienced abnormal or increased hidrosis during mastication, compared to the preoperative situation.
The POSAS was used to assess both the participant’s and the examiner’s satisfaction with the scar. The examiner collecting the data was trained in using the POSAS by an oral and maxillofacial surgeon familiar with the tool; this examiner(MA) was the sole examiner for all in-person assessments. For each patient, the examiner assigned a score from 0 to 9 for each element of the easy-to-use tool, then summed and averaged the individual scores to generate a final score between 0 and 9.
Overall patient satisfaction was measured objectively by asking patients “on a Likert scale of 1 to 10, how satisfied are you with your surgery, including the presurgical care, the surgery itself, and the postsurgical care and results?”
Data Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS), version 27 (IBM, Armonk, NY), with significance level set at p < 0.05 (2-tailed). Data were checked for normality. Differences between the TP and SM groups were analyzed using the Mann–Whitney U test for continuous variables or the χ2 test for categorical variables (or the Fisher exact test when more than 20% of the cells contained expected frequencies of less than 5).
Results
A total of 275 patients presented to the study hospital with condylar fracture during the study period. Of these, 32 met the eligibility criteria and were included in the chart audit, as outlined in Fig. 3. Fourteen of these patients were available to attend an in-person assessment, all between 1 and 7 years from the date of their surgery.
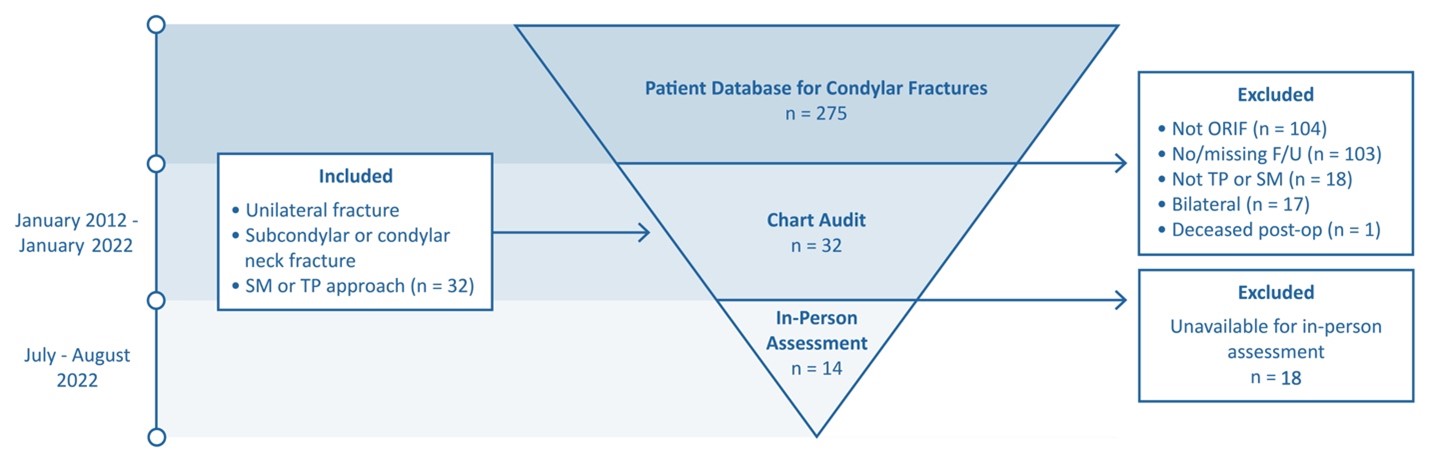
Figure 3: Study design and participant selection process. The cause of the sole postoperative death was due to complications unrelated to treatment of condylar fracture. F/U = follow-up; ORIF = open reduction and internal fixation; post-op = postoperatively; SM = submandibular; TP = transparotid.
The characteristics of the study participants are summarized in Table 2. The median age of participants was 37.0 years (range 14 to 68 years). The majority were male (88%), most presented with subcondylar fractures (88%), and most required 2 plates (94%). Left and right fractures were about equally represented. Most participants self-reported that they smoked (63%) and consumed alcohol (80%). None of these factors differed significantly between the SM and TP groups (p > 0.05), which indicated a lack of confounding factors for these variables within our sample.
|
Characteristic |
Group; no. (%) of patientsa,b |
p value |
||
|---|---|---|---|---|
|
All n = 32 (100) |
Submandibular approach |
Transparotid approach |
||
|
Note: NA = not applicable. |
||||
| Age (years) | 0.69 | |||
| Median | 37.0 | 36.0 | 38.5 | |
| Range | (14–68) | (19–68) | (14–61) | |
| Sex | 0.61 | |||
| Male | 28 (88) | 15 (54) | 13 (46) | |
| Female | 4 (12) | 3 (75) | 1 (25) | |
| Side | 0.69 | |||
| Left | 17 (53) | 9 (53) | 8 (47) | |
| Right | 15 (47) | 9 (60) | 6 (40) | |
| Location | > 0.99 | |||
| Subcondylar | 28 (88) | 16 (57) | 12 (43) | |
| Condylar neck | 4 (12) | 2 (50) | 2 (50) | |
| No. of plates | > 0.99 | |||
| 1 | 2 (6) | 1 (50) | 1 (50) | |
| 2 | 30 (94) | 17 (57) | 13 (43) | |
| Smoking habit | 0.20 | |||
| Yes | 20 (62) | 13 (65) | 7 (35) | |
| No | 12 (38) | 5 (42) | 7 (58) | |
| Alcohol consumptionc | > 0.99 | |||
| Yes | 24 (80) | 14 (58) | 10 (42) | |
| No | 6 (20) | 4 (67) | 2 (33) | |
| Diabetes mellitus (type 1 or type 2) | NA | |||
| Yes | – | – | – | |
| No | 32 (100) | 18 (56) | 14 (44) | |
Table 3 outlines the data collected from the chart audit portion of our study. The outcomes of MIIO, paresthesia, motor weakness and change in occlusion were similar with the SM and TP approaches (p > 0.05). No postoperative infection was reported for any patient in either group.
|
Characteristic |
Group; no. (%) of patientsa,b |
p value |
||
|---|---|---|---|---|
|
All n = 32 (100) |
Submandibular approach |
Transparotid approach |
||
|
Note: NA = not applicable; SD = standard deviation. |
||||
| Maximum interincisal opening (mm), mean ± SD | 27.2 ± 8.4 | 26.1 ± 8.0 | 28.3 ± 9.2 | 0.58 |
| Paresthesia | 0.67 | |||
| No | 26 (81) | 14 (54) | 12 (46) | |
| Yes | 6 (19) | 4 (67) | 2 (33) | |
| Motor weakness | 0.10 | |||
| No | 27 (84) | 13 (48) | 14 (52) | |
| Yes | 5 (16) | 5 (100) | 0 (0) | |
| Infection | ||||
| No | 32 (100) | 18 (56) | 14 (44) | NA |
| Yes | – | – | – | |
| Change from preoperative occlusion | > 0.99 | |||
| Grade 1 | 27 (84) | 15 (56) | 12 (44) | |