Abstract
Objectives:
The diagnosis, symptom onset, treatment, prognosis, radiographic features and effect of litigation on patients suffering temporomandibular disorders (TMDs) following motor vehicle accidents (MVAs) are still unknown yet highly debated. This review summarizes literature on this topic and provides evidence-based guidance to dental practitioners.
Methods
We applied PRISMA guidelines and their extension for scoping reviews (PRISMA-ScR). The search strategy was defined, and the electronic search included PubMed, MEDLINE, EMBASE, Cochrane Library, Web of Science, and Scopus. Extracted data were organized into categories, and we present a narrative summary of the main findings.
Results:
We included 37 articles in the review: 15 assessed the diagnosis of TMD following an MVA; 6 assessed onset of symptoms; 13 analyzed treatment options; 10 reviewed prognosis; 6 reviewed imaging findings; and 4 reviewed litigation factors.
Conclusions:
The review revealed heterogeneous results regarding the diagnosis, treatment, prognosis, imaging and litigation factors in MVA-related TMD patients. Future studies are recommended, and no definitive conclusions were drawn.
Introduction
Motor vehicle accidents (MVAs), defined as collisions involving motor vehicles with other vehicles, pedestrians, animals or stationary objects, are known to cause a variety of injuries, including whiplash-associated disorders (WADs). Whiplash is characterized by a sudden, forceful back-and-forth movement of the neck, which is frequently associated with the onset of symptoms of temporomandibular disorder (TMD).1,2 The prevalence of TMD after an MVA is reported to be significantly higher than that in the general population not involved in MVAs, with a notable incidence of TMD in those reporting a history of whiplash.3,4 In 2022, Canada saw an increase in the number of fatalities, serious injuries and total injuries from MVAs compared with the previous year. Despite this, there has been a long-term decline in the number of MVAs resulting in a single injury but no fatalities: from 150 493 in 2003 to 89 787 in 2022. The most frequent occurrences of serious injuries and fatalities were among people aged 25–34 years.1,5
The interrelation between TMDs and MVAs remains a subject of both medical and legal debate, compounded by the inherent variability in symptom presentation and the multifactorial nature of treatment approaches. This complexity is further amplified by significant legal implications, particularly concerning the future care costs and litigation in some Canadian provinces.
TMD encompasses a spectrum of over 30 clinical conditions affecting the temporomandibular joint (TMJ) and associated musculature. These conditions are generally classified into 3 primary categories: joint disorders, masticatory muscle disorders and TMD-related headaches.6 The pathophysiology of MVA-related TMD may involve both direct mechanical trauma to the TMJ and indirect effects, such as changes in the central nervous system, with psychological stress playing a contributory role.2,7
In addition to the indirect trauma associated with whiplash during MVAs, patients may also experience direct trauma from various internal and external sources, such as airbags, seatbelts and other components of the vehicle, as well as external objects, such as poles and roads.8 This scoping review seeks to consolidate and evaluate the existing literature on the nexus of TMD and MVAs concerning diagnosis, symptom onset, radiographic presentation, treatment modalities, prognostic outcomes and litigation, thereby informing the broader medical, dental and legal communities on optimal management strategies for this patient group.
Methods
Our study population included all patients aged ≥18 years, who had been involved in an MVA. All settings of MVA accidents and patient complaints were included, i.e., patients seen in all clinical contexts (medical and dental settings). There was no restriction on geographic location.
The databases PubMed, EMBASE, Web of Science, Cochrane and Scopus were queried. Types of studies included were experimental, observation and reviews. There was no limit on articles by date, but only articles published in English were used. The review was registered with PROSPERO (ID CRD42023400003).
Terms used in the search strategy were: (motor* OR vehicle* OR automobile* OR car OR cars OR truck* OR traffic) adj3 (accident* OR collision* OR crash*) AND temporomandibular OR temporo mandibular
On 28 May 2023, we identified 400 articles from Scopus, 285 from MEDLINE, 145 from PubMed, 505 from Embase, 322 from Web of Science and 7 from Cochrane. All articles were uploaded to Covidence (Melbourne, Australia) for organization and screening. After removing duplicates, 697 articles were screened for relevance using titles and abstracts independently by NB and KP. RF resolved any conflicts. A total of 141 full-text articles were then independently reviewed by authors NB and KP, and 37 articles were included (Figure 1).
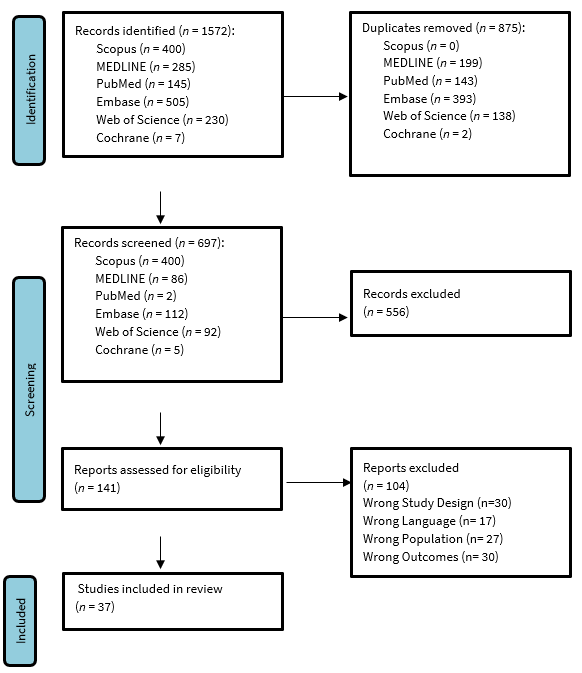
Figure 1: PRISMA flowchart of search strategy and results.
Results
The 37 articles analyzed in this review were categorized according to their primary focus among the search objectives, although several articles addressed more than 1 of the 6 areas of interest. Table 1 illustrates the distribution of articles across these outcomes: 15 articles were concerned with diagnosis,4,9–22 6 with symptom onset,23–28 13 with treatment options,15,16,18,24–26,29–35 10 with prognosis,13,24–26,29,36–40 6 with radiographic features40–45 and 5 with litigation factors.21,25,31,38,43 Some articles contributed to multiple outcomes. Relevant findings from each article were systematically highlighted and are detailed in Tables 2–7.
|
Topic |
Included articles |
|---|---|
| Diagnosis of TMD (n = 15) | Abd-Ul-Salam et al. 20029 Bal et al. 202010 Häggman-Henrikson et al. 201611 Eklund et al. 202012 Fernandez et al. 2009 13 Häggman-Henrikson et al. 20144 Klobas et al. 200414 Krogstad et al. 199815 Kronn 1993 16 Lampa et al. 2017 17 Landzberg et al. 2017 18 Marini et al. 2013 19 McKay & Christensen 199820 Ferrari et al. 1999 21 Visscher et al. 200522 |
| Onset of symptoms (n = 6) | Al-Ani 202323 Corsalini et al. 202224 Epstein & Klasser 201125 Epstein et al. 201026 Salé & Isberg 200727 Severinsson et al. 201028 |
| Treatment of TMD (n = 13) | Corsalini et al. 202224 Epstein 199229 Epstein & Klasser 201125 Epstein et al. 201026 Klobas et al. 200630 Kolbinson et al. 199731 Krogstad et al. 199815 Kronn 199316 Landzberg et al. 201718 Moses & Skoog 198632 McNamara et al. 199633 Naqvi & Fating 202034 Romanelli et al. 199235 |
| Prognosis of TMD (n = 10) | Böthun et al. 202336 Corsalini et al. 202224 Epstein 199229 Epstein & Klasser 201125 Epstein et al. 201026 Fernandez et al. 200913 Kasch et al. 200237 Kolbinson et al. 199838 Lampa et al. 202039 Salé et al. 201440 |
| Radiographic features of TMD (n = 6) | Ferrari & Leonard 199841 Garcia & Arrington 199642 Grushka et al. 200743 Lee et al. 201844 Lee et al. 202145 Salé et al. 201440 |
| Litigation factors (n = 5) | Epstein & Klasser 201125 Ferrari et al. 199921 Grushka et al. 200743 Kolbinson et al. 199731 Kolbinson et al. 199838 |
|
Authors, year, country |
Setting, study design |
Key findings |
|---|---|---|
|
Note: MVA = motor vehicle accident, TMD = temporomandibular disorder, TMJ = temporomandibular joint, WAD = whiplash associated disorder. |
||
| Abd-Ul-Salam et al. 2002, Canada9 |
Dental school/hospital Retrospective review Arthroscopic findings in patients with whiplash injury |
Disc displacement without reduction was common in WAD patients. Synovitis occurred in 73% of the patients, but severe synovitis was rare (7%). Mild to severe adhesions in 67% of joints. |
| Bal et al. 2020, Turkey10 |
Orofacial pain clinic at Yeditepe University Faculty of Dentistry Retrospective review Trauma and whiplash effect on clicking and crepitation |
Direct and/or whiplash trauma was not associated with TMDs or TMJ sounds, such as clicking/crepitation. |
| Häggman-Henrikson et al. 2016, Sweden11 |
Umeå University Hospital Cross-sectional study Comparing pain between patients with or without trauma |
Jaw pain, pain on movement and jaw locking were commonly seen in patients suffering from neck trauma. |
| Eklund et al. 2020, Sweden12 |
Umeå University Hospital Randomized controlled trial Comparing jaw and head/neck amplitude between whiplash and non-whiplash groups |
Compared with controls, WAD cases showed smaller jaw movement amplitude and higher neck pain intensity. High neck pain cases had significantly smaller jaw movement amplitudes. |
| Fernandez et al. 2009, USA13 |
Literature review Comparing traumatic and non-traumatic TMD patients |
Increased incidence of limited jaw mobility, masticatory muscle tenderness and internal derangement found in MVA cases. |
| Häggman-Henrikson et al. 2014, Sweden4 |
Systematic review Prevalence and sign/symptoms of TMD following MVA |
Compared with patients with TMD localized to the facial region, TMD patients with a history of whiplash trauma reported more TMD symptoms (limited jaw opening, increased TMD pain, headaches and stress). |
| Klobas et al. 2004, Sweden14 |
Public dental clinic Cross-sectional study Questionnaire and clinical exam evaluating TMJ in patients with chronic WAD and control |
TMD symptoms (limited opening, pain to palpation, TMJ clicking) were significantly higher in WAD group compared with the control group. |
| Krogstad et al. 1998, Norway15 |
Orofacial pain clinic Cross-sectional study Compare psychological and physical distress in whiplash patients receiving treatment |
WAD patients had higher scores than the non-traumatic TMD patients regarding obsession, somatization, depression and anger/hostility. |
| Kronn 1993, Ireland16 |
Accident and Emergency Department, St James’ Hospital Cross-sectional study Cervical whiplash patients compared with control patients |
TMJ pain (p < 0.001) and limitation of mouth opening (p < 0.01). were significantly more frequent in the WAD group. Joint sounds and jaw deviation were not significantly different between groups. |
| Lampa et al. 2017, Sweden17 |
Emergency department at Umeå University Hospital Cross-sectional study Compare whiplash-related TMD to control patients |
WAD patients show signs of impaired chewing capacity as indicated by susceptibility to earlier onset of fatigue and pain while chewing during acute stages. |
| Landzberg et al. 2017, USA18 | Narrative review | Among TMD sufferers, jaw pain and dysfunction were more severe in those with a history of cervical whiplash. |
| Marini et al. 2013, Italy19 |
Department of Orthodontics and Gnathology, University of Bologna, Italy Case–control study Compare the frequency of specific TMD diagnoses in patients who had late whiplash syndrome and control group |
Prevalence of myofascial pain and disc displacement with reduction was significantly higher in patients after MVA who experienced orofacial pain than in patients with chronic orofacial pain who had no history of MVA. No significant differences between patients after MVA and control patients concerning the frequency of osteoarthritis or disc displacement without reduction. |
| McKay & Christensen 1998, USA20 | Narrative review | TMJ disc displacement and inflammation following MVA often represent pre-existing disease entity that MVA exacerbates. |
| Ferrari et al. 1999, Lithuania21 |
Traffic police department of Kaunas, Lithuania Retrospective study Rear-end collision patients compared with controls |
Both groups exhibited similar frequency of jaw pain. Both groups exhibited a low prevalence of joint sounds, jaw locking, tinnitus and facial pain. |
| Visscher et al. 2005, Netherlands22 |
Roessingh Rehabilitation Center Cross-sectional study Comparison of WAD pain group and control group with no neck pain |
WAD pain group more often suffered from TMD pain and widespread pain than the no-neck-pain group. WAD patients exhibited greater psychological distress. |
|
Authors, year, country |
Setting, study design |
Key findings |
|---|---|---|
|
Note: MVA = motor vehicle accident, TMD = temporomandibular disorder, TMJ = temporomandibular joint, WAD = whiplash associated disorder. |
||
| Al-Ani 2023, UK23 | Narrative review | Click development after an accident is common and correlated with functional limitation. TMD symptoms might not become apparent until pain from other structures subsides (3–4 weeks). Other symptoms can mask TMD symptoms. |
| Corsalini et al. 2022, Italy24 | Dental Prosthesis Department, University of Bari Prospective clinical study Patients examined at multiple time points after MVA | Patients often perceive no pain or injury immediately after MVA. Symptomatology gradually increases in the following days. |
| Epstein & Klasser 2011, USA25 | Narrative review | Evidence for delayed onset/recognition of TMD after whiplash is grade B. |
| Epstein et al. 2010, USA26 | Narrative review | Incidence of new symptoms of TMDs among MVA patients was 5 times that of control group and higher in females than males. Delated painful symptoms at 1-year follow up were seen in 19%. |
| Salé & Isberg 2007, Sweden27 | Hospital emergency department Controlled prospective study 60 patients assessed and examined before whiplash and multiple time points after | 33% of whiplash sufferers are at risk of developing delayed TMJ pain and dysfunction with onset during the year after the accident. |
| Severinsson et al. 2010, Sweden28 | Emergency hospital departments, primary health clinics and Volvo accident investigation team Controlled prospective study Assessment of jaw pain following MVA | Jaw symptoms are uncommon in the acute phase following MVA, but frequently develop over months after an accident. Women have symptoms more often than men. Symptoms after low-impact rear-end accidents are common. |
|
Authors, year, country |
Setting, study design |
Key findings |
|---|---|---|
|
Note: MVA = motor vehicle accident, NSAID = nonsteroidal anti-inflammatory drug, TENS = transcutaneous electrical nerve stimulation, TMD = temporomandibular disorder, TMJ = temporomandibular joint, WAD = whiplash associated disorder. |
||
| Corsalini et al. 2022, Italy24 |
Dental prosthesis department, University of Bar Prospective clinical study Use of Zimmer collar use and occlusal splint |
Patients who used occlusal splint therapy as a stand-alone treatment, and did not use pharmacologic intervention showed the worst outcomes. |
| Epstein 1992, Canada29 | Narrative review |
The effect of occlusal appliances in reducing pain associated with TMD is well documented. No evidence to support the suggestion that structural changes (e.g., occlusal treatment or surgery) are required in TMD management. |
| Epstein & Klasser 2011, USA25 | Narrative review | Multiple therapeutic approaches exist for TMD, including NSAIDs, psychotropic agents, steroids and anesthetics. Prednisone is mentioned as an option for acute management, while intramuscular injections are noted for chronic cases. Evidence for muscle relaxants and analgesics remains limited. |
| Epstein et al. 2010, USA26 | Narrative review |
Prednisone can be used for acute pain within 1 week of injury. For chronic symptoms, intramuscular lidocaine was superior to placebo. Myofascial trigger point injection was effective, but no difference was documented between saline and botulinum toxin. Limited evidence for pharmacotherapy. |
| Klobas et al. 2006, Sweden30 |
Rehabilitation centre Case–control study 55 patients diagnosed with chronic TMD and WAD; 25 underwent jaw exercises and 30 followed regular rehab |
Jaw exercises did not help chronic whiplash TMD patients’ pain complaints but did improve range of motion. |
| Kolbinson et al. 1997, Canada31 |
Oral medicine private practice Cross-sectional study Comparing treatments and their success in TMD patients with and without MVA |
MVA patients tended to receive more types of treatment over a longer period and have poorer treatment outcomes compared with the non-trauma group. |
| Krogstad et al. 1998, Norway15 |
Cross-sectional study Compare somatic complaints and psychological distress in a group of whiplash patients and examine the effects of conservative treatments. |
Treatment focused on the entire body musculature with cognitive and behavioural approaches best. Conservative treatment does not appear to have a clear positive influence on patients’ headache frequency and intensity. |
| Kronn 1993, Ireland16 |
Accident and emergency department, St James’ Hospital Cross-sectional study 40 consecutive patients with a cervical whiplash injury were examined and compared with 40 matched controls |
WAD group is more likely to seek treatment for their symptoms compared with controls. |
| Landzberg et al. 2017, USA18 | Narrative review |
Traditional treatments tend to work more poorly in patients with a history of whiplash. A multidisciplinary approach, including psychological evaluation, is recommended. |
| McNamara et al. 1996, Australia33 |
Case–control study Comparison between MVA and control groups with TMD response to arthroscopic treatment |
Arthroscopic surgery reduced pain for both groups. |
| Naqvi & Fating 2020, India34 |
Case study 1 patient with 3-year history of TMD symptoms following MVA |
Physiotherapy (TENS, myofascial release and isometric exercises) can help improve range of motion and reduce pain. |
| Romanelli et al. 1992, Canada35 |
Craniofacial pain clinical research unit, Mount Sinai Hospital Retrospective study Comparison of various treatment modalities |
Mandibular bite plane (splint) saw 73% improvement in symptoms for non-MVA and 43% for MVA patients. Physiotherapy saw 74% improvement in symptoms for non-MVA and 64% for MVA patients. NSAID saw 76% improvement in symptoms for non-MVA and 76% for MVA patients. Moist heat and massage saw 77% improvement in symptoms for non-MVA and 59% for MVA patients. Overall more success in modalities when no MVA history. |
|
Authors, year, country |
Setting, study design |
Key findings |
|---|---|---|
|
Note: MVA = motor vehicle accident, TMD = temporomandibular disorder, TMJ = temporomandibular joint, WAD = whiplash associated disorder. |
||
| Böthun et al. 2023, Sweden36 |
Emergency department Case–control study Pain on palpation on neck muscles, jaw muscles and jaw movements post whiplash |
Individuals with whiplash trauma present a higher risk for short-term and long-term jaw pain but exhibit normal jaw movements. Women have a worse prognosis than men. |
| Corsalini et al. 2022, Italy24 |
Dental prosthesis department, University of Bar Prospective clinical study Craniomandibular dysfunction indices |
Acute WAD disorders are often self-limiting over a few months.
Symptom chronicity appears mostly related to lesion severity, possible pre-existence of craniomandibular dysfunction/disorder and patient age. |
| Epstein 1992, Canada29 | Narrative review |
Statistically significant prognostic factors for MVA-related TMD include rear and front collision, occipital headache, referred symptoms, intracapsular pain/headache, abnormal neurology, positive radiology, osteoarthrosis and insurance claims. Trauma-associated TMD vs non-trauma associated TMD responds less well to therapy. Clicking resolves in 25% of MVA patients. 70% of patients with non-painful clicking will develop pain. |
| Epstein & Klasser 2011, USA25 | Narrative review | Many factors affect prognosis including pre-existing history, physical and psychological factors. |
| Epstein et al. 2010, USA26 | Narrative review |
Approximately 15–40% of patients with acute WAD develop chronic symptoms. Both groups (WAD and non-WAD) responded equally well to conservative treatment. |
| Fernandez et al. 2009, USA13 | Narrative review | Thorough, comprehensive assessment required in MVA patients. Balance and postural abnormalities, shoulder-neck headache, stress habits and centrally mediated pain factors should be included as potential variables of prognosis. |
| Kasch et al. 2002, Denmark37 |
Case–control study Assess TMJ pain in post-MVA patients |
Global pain intensity was low after 4 weeks and 6 months post-injury (McGill Pain Questionnaire and exam by dentist), suggesting whiplash is not a major risk factor in the development of TMD issues. |
| Kolbinson et al. 1998, Canada38 |
Private oral medicine practice Retrospective review 50 patients with post-motor vehicle accident TMD |
Significant predictors of the number of treatment visits were the severity of vehicle damage, headrest use, position in the vehicle and insurance claim status. Impact direction and number of MVAs were significant predictors of neck muscle tenderness scores. The severity of vehicle damage and patient age were significant predictors of final jaw muscle tendern… 
|