
Abstract
Background: In Canada, although the incidence of smoking-related oral cavity cancers has decreased, oropharyngeal cancers associated with human papilloma virus (HPV) are on the rise. During their routine interactions with patients, dentists have the opportunity to intervene. This study was conducted to assess dentists’ capacity to prevent and detect oral cancers and to identify the barriers and facilitators that affect this capacity.
Methods: A 25-item, self-administered questionnaire was emailed to Ontario dentists through their regulatory body. It aimed to assess their perceptions about various aspects of oral cancer prevention and detection, including their knowledge, attitudes and practices. A binary logistic regression model was constructed for each modifiable risk factor (smoking, alcohol use, HPV) to identify the predictors of dentists’ readiness to discuss with patients the connection between risk factors and oral cancers.
Results: Of the 9975 dentists contacted, 932 completed the survey. Most respondents (92.4%) believed that they are adequately trained to recognize the early signs and symptoms of oral cancer. However, only 35.4% of respondents said that they are adequately trained to obtain biopsy samples from suspected lesions. In addition, only a small proportion (< 40%) of the dentists believed that they are adequately trained to address relevant risk factors. Compared with dentists who said that they are adequately trained and currently assess a given risk factor, the odds of discussing the risk factor were consistently and significantly lower among those who said that they are inadequately trained (OR: smoking 0.11, alcohol 0.52, HPV 0.36) and among those who do not currently assess that risk factor (OR: smoking 0.12, alcohol 0.22, HPV 0.23).
Conclusions: This study suggests that the capacity of Ontario dentists to detect and prevent oral cancers is limited by lack of training in using oral cancer screening tools and addressing risk factors. To mitigate this barrier, dentists’ capacity could be enhanced by improving their training in detecting oral cancers and their readiness to assess and address the risk factors.
Oral cancers, including oral cavity cancers (OCCs) and oropharyngeal cancers (OPCs), represent a public health problem because of their substantial impact at individual, societal and health care system levels.1-6 Public health efforts in tobacco control have not significantly changed the overall incidence of oral cancers in high-income countries, such as Canada, because of the increased incidence of OPCs linked to human papilloma virus (HPV) types 16 and 18.6-9 In Canada, the incidence of OPCs linked to HPV has been increasing, especially among men: from 4.1 per 100 000 in 1997 to 6.4 per 100 000 in 2012.11 In contrast, the incidence of OCCs has decreased over the same period from 6.2 to 4.2 per 100 000. This decrease has been mostly attributed to declining smoking prevalence (from 25.2% in 1999 to 13.0% in 2015) among Canadians aged 15 years old and over.10,11
The epidemiology of oral cancers varies by sociodemographic factor and anatomical location. People who are at risk of developing OPCs tend to be white, non-smokers and relatively younger men from higher socioeconomic levels compared with those at risk of developing OCCs.12 Recent studies suggest that although OPC rates are lower among women, the incidence of OPC is increasing among certain subgroups.13 Anatomically, the tongue and floor of the mouth are the most common sites for OCCs, whereas the posterior third of the tongue, tonsils and medial wall of the pharynx are commonly involved in OPCs.7,8,12 Etiology is multifactorial and varies by the type of site involved; for example, smoking and alcohol use are more closely related to OCCs, whereas HPV-related oral infections progress more commonly as OPCs.7,8,12
Oral cancers are commonly diagnosed in advanced stages, which may adversely affect survival rates, metastasis, recurrence rates and treatment costs.3,14,15 The transformation of oral epithelial cells from normal or premalignant to malignant is multifactorial and unpredictable; therefore, all lesions require follow up, and innovative methods for effective prevention and intervention are needed.16 The available limited evidence also suggests that the burden of the potential consequences could be alleviated by early detection and diagnosis.17,18
The fact that more than half of oral cancers are diagnosed at an advanced (regional or distant) stage15 is largely attributed to patients reporting late because of cognitive and psychosocial factors. This highlights the need to increase the capacity of health care providers, particularly dentists, to increase patients’ awareness and to detect the signs of unreported premalignant and malignant oral lesions during routine oral examinations.19-27 However, a significant percentage of dentists do not provide oral cancer screening routinely for all patients, especially at recall visits, and they typically do not palpate lymph nodes during screening.28-34 Moreover, previous research also shows a lack of knowledge among dentists regarding the most common sites for oral cancers.34-37 Recent studies have suggested that dentists’ practices regarding oral cancer detection have not changed much over time.38-40
Dentists can augment their role in detecting oral cancers by assessing the risk among their patients and identify and target those at high risk with preventive interventions to minimize the future burden.41 Compared with physicians, dentists are less likely to assess past and present alcohol and tobacco use, particularly the types of each and amounts consumed.29,34,36 Also, in their routine practices, only a small percentage of dentists discuss and address HPV as a risk factor with patients.42,43 More important, the vast majority of dentists report feeling inadequately trained to address the risk factors for both OCCs and OPCs.28,36,38
Improving the capacity of dentists to reduce the burden of oral cancers requires identifying the barriers that affect their capacity to prevent and detect these diseases, combined with understanding the relevant and preferred sources of information and delivery. Therefore, the objective of this study was to assess this capacity as well as the barriers and facilitators that may be targeted to expand it.
Methods
Survey Instrument
This study was based on 18 sociodemographic items in a 25-item, self-administered questionnaire that was developed based on a comprehensive literature review and feedback from clinical dentists specializing in oral cancers, experts in the field of HPV and public health experts (Appendix A – available upon request).35,42,43 The extracted items were pilot tested among 10 Ontario dentists and revised based on their feedback. A public link to the survey was generated and shared with the Royal College of Dental Surgeons of Ontario (RCDSO, the regulatory body for Ontario dentists). The RCDSO emailed the link to its members (9975 practising dentists) on 2 August 2017. The dentists were asked to complete the online survey within 4 weeks; email reminders were sent at 2 and 3 weeks (16 and 23 August 2017).
The respondents’ capacity to detect oral cancers was measured by their survey responses to 5 items related to frequency of oral cancer examination, anatomical structures screened, ability to recognize signs and symptoms, confidence in the use of screening tools and adequacy of relevant training (items 1, 5–7 and 10). Also, 3 items explored respondents’ perceived barriers to and facilitators of oral cancer screening and their preferred format for continuing dental education (items 8, 9 and 18).
The respondents’ capacity to prevent oral cancers was measured based on 2 items related to their knowledge of risk factors, adequacy of training to provide counseling regarding cessation of tobacco and/or alcohol use and HPV vaccine counseling/recommendation (items 2 and 10). In addition, items 3 and 4 measured dentists’ readiness to evaluate and discuss oral cancers and patient-reported risk factors and behaviours during the medical history interview.
The stage-of-change construct from the transtheoretical model (TTM) was used to assess dentists’ readiness to discuss behaviours related to high risk of oral cancers, such as alcohol and/or tobacco use and HPV infection/vaccination with patients. Respondents selecting “Yes, with all patients” or “Yes, but with some patients” were assigned to the action stage, and participants responding “No, but I have thought about it” (contemplation) and “No, and I have no plans to start” (pre-contemplation) were assigned to the pre-action stage.42,44
Statistical Analyses
We used descriptive analysis to assess the number and proportion of the sample responding to each survey item. A binary logistic regression model was constructed for each modifiable risk factor (smoking, alcohol use, HPV) to estimate the impacts of sociodemographic characteristics, readiness to assess the specified risk factor, adequacy of training to address the risk factor and the effect of perception of the risk factor on respondents’ readiness to discuss with patients the connection between the risk factor and oral cancers. SPSS software, version 24 was used for all statistical analyses.
Ethics review
Ethics approval for conducting this survey was obtained from the Research Ethics Board of Public Health Ontario (file 2017-040.01). A statement was included in the survey questionnaire to record the active consent of participants.
Results
Of the 9975 dentists contacted, 932 completed the survey for a participation rate of 9.3%. To ensure participants’ privacy, sociodemographic subcategories containing 5 or fewer respondents were not included in the final analyses unless the data could be combined with other subcategories. Table 1 presents the sociodemographic characteristics of the dentists included in the final analyses (n = 932). Most respondents were male (57.0%), primarily general dentists in private practice (84.1%) and practising in an urban area (66.9%). Approximately 60% of respondents were Canadian trained, and about 65% reported practising in Canada for 10 years or more. Most respondents reported attending a continuing education course on oral cancers either within the past year (33.8%) or during the past 2–5 years (40.3%).
Through personal communication, data (not shown) were received from the RCDSO, indicating that the sociodemographic profiles of the survey respondents were not significantly different from those of all dentists registered in Ontario in terms of age, gender and training.
|
Characteristic |
No. (%) |
|---|---|
| * Missing data, as not all participants shared their complete demographic information
^ Other includes dental school faculty/staff member, uniformed services/federal employee, provincial or municipal employee, hospital staff dentist and graduate student/resident in a specialty training program. |
|
| Gender | |
| Male | 527 (57) |
| Female | 405 (43.0) |
| Age (n = 926)* | |
| 20–29 years | 36 (3.9) |
| 30–39 years | 217 (23.4) |
| 40–49 years | 219 (23.7) |
| 50–59 years | 244 (26.3) |
| ≥ 60 years | 210 (22.7) |
| Practice type (n = 929)* | |
| Private practice general practitioner | 781 (84.1) |
| Private practice specialist | 95 (10.2) |
| Other^ | 53 (5.7) |
| Office location (n = 924)*† | |
| Urban area | 618 (66.9) |
| Suburban area | 210 (22.7) |
| Rural area | 96 (10.4) |
| Training | |
| Canadian trained | 553 (59.8) |
| United States trained | 102 (11.0) |
| Internationally trained with direct licensure | 139 (15.0) |
| Internationally trained and attended a qualifying program | 111 (12.0) |
| Prefer not to answer | 20 (2.2) |
| Years practising in Canada (n = 925)* | |
| < 1 year | 60 (6.5) |
| 1 to < 3 years | 90 (9.7) |
| 3 to < 5 years | 75 (8.1) |
| 5 to < 10 years | 97 (10.5) |
| ≥ 10 years | 602 (65.2) |
| Last continuing education course attended on oral cancer (n = 923)* | |
| Within the past year | 312 (33.8) |
| During the past 2–5 years | 372 (40.3) |
| More than 5 years ago | 123 (13.3) |
| Never | 49 (5.3) |
| Have yet to attend | 45 (4.9) |
| Do not know | 22 (2.4) |
Dentists’ Capacity to Detect Oral Cancers
Frequency of oral cancer examinations: Most participants reported always or very frequently providing oral cancer examinations to all high-risk age groups (> 45 years), although a larger proportion reported doing so while conducting a complete examination than during a recall examination (Table 2).
|
Type of oral examination |
Age group, years |
Always/very frequently, no. (%) |
Occasionally/rarely, no. (%) |
I do not see this age group, no. (%) |
|---|---|---|---|---|
| *Total responses vary because of missing data. | ||||
| Complete | 0–8 | 489 (55.0) | 349 (39.3) | 51 (5.7) |
| 9–26 | 741 (83.2) | 146 (16.4) | 4 (0.4) | |
| 27–45 | 815 (91.4) | 67 (7.5) | 10 (1.1) | |
| 46–64 | 844 (94.3) | 42 (4.7) | 9 (1.0) | |
| 65+ | 836 (93.3) | 41 (4.6) | 19 (2.1) | |
| Recall | 0–8 | 350 (50.9) | 305 (44.3) | 33 (4.8) |
| 9–26 | 514 (76.7) | 151 (22.5) | 5 (0.7) | |
| 27–45 | 567 (85.0) | 91 (13.6) | 9 (1.3) | |
| 46–64 | 596 (89.1) | 65 (9.7) | 8 (1.2) | |
| 65+ | 594 (88.4) | 61 (9.1) | 17 (2.5) | |
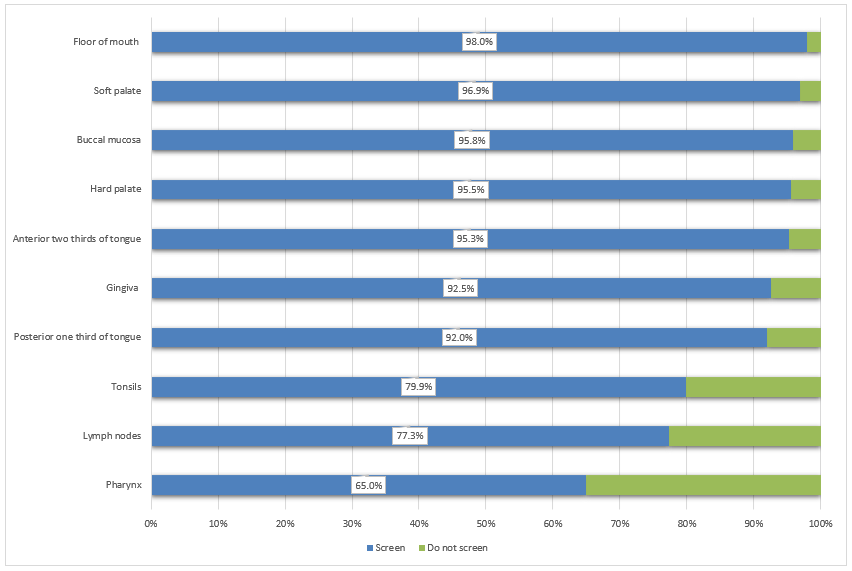
Anatomical sites screened: During the oral examination, most of the respondents (more than 90%) screen the gingivae, buccal mucosa, and anterior 2-thirds and posterior 1-third of the tongue (Fig. 1). Comparatively fewer respondents examine the anatomical structures in the oropharyngeal area, including the tonsils (79.9%), lymph nodes (77.3%) and pharyngeal area (65.0%).
Figure 1: Proportion of dentists who screen each anatomical structure (n = 932).
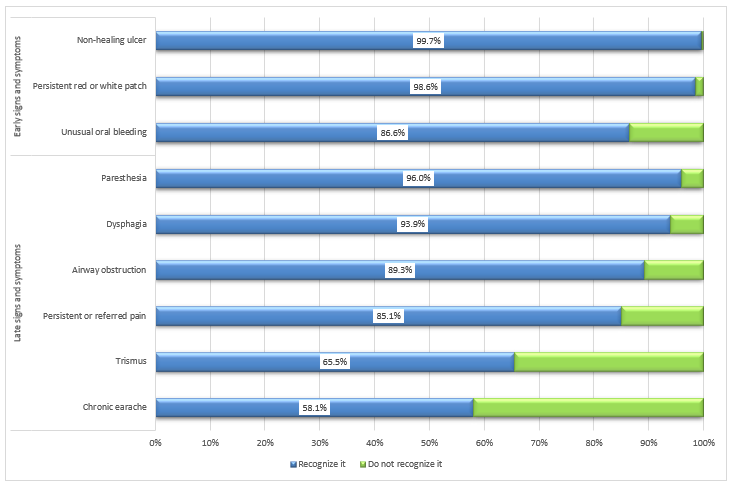
Recognizing signs and symptoms: A large proportion of dentists reported recognizing common signs and symptoms of oral cancers, including non-healing ulcers (99.7%), the presence of a persistent white or red patch (98.6%) and unusual bleeding (86.6%) (Fig. 2). However, they found recognition of late-stage signs and symptoms more challenging; specifically, fewer participants selected chronic earache (58.1%) and trismus (65.5%) as late-stage oral cancer symptoms.
Figure 2: Proportion of dentists who recognize oral cancer signs and symptoms (n = 932).
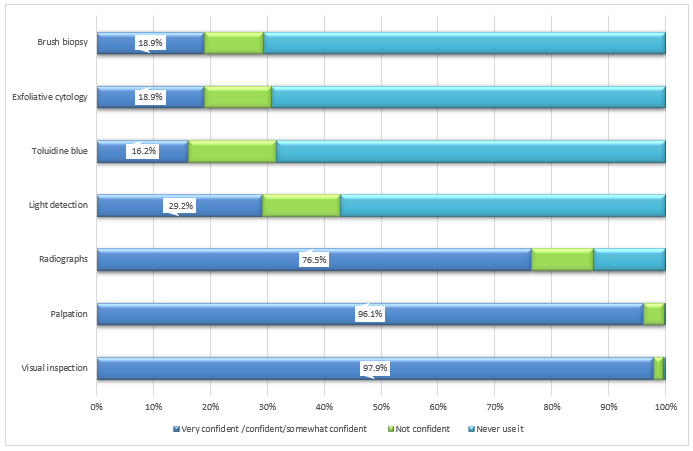
Use of screening tools: Participants showed varying levels of confidence in using oral cancer screening tools: visual inspection (97.9%), palpation (96.1%) and radiographs (76.5%) (Fig. 3). Fewer participants reported feeling confident or somewhat confident in their use of light detection using fluorescence visualization (29.2%), exfoliative cytology (18.9%), brush biopsy (18.9%) and toluidine blue dye (16.2%).
Figure 3: Dentists’ confidence in using various oral cancer screening tools (n = 932).
Adequacy of relevant training in detection of oral cancers: Most respondents agreed or strongly agreed that their training in detecting the early signs and symptoms of oral cancers is adequate (92.4%). In contrast, only 35.4% of respondents agreed or strongly agreed that they are adequately trained to obtain biopsy samples from suspected lesions.
Barriers to and facilitators of providing oral cancer examinations: Respondents cited 3 major barriers to performing regular oral cancer examinations on all patients (Table 3): the lack of a separate oral cancer examination fee code (30.4%), lack of clinical guidelines from professional dental organizations (20.2%) and lack of comfort in palpating patients’ lymph nodes (13.0%).
The major facilitators of regular oral cancer examinations included more efficient screening tools (75.2%), less expensive screening tools (73.2%) and more training in oral cancer examinations (70.6%) (Table 3). The expressed preferences for future oral cancer screening and detection education included lectures (53.6%) and hands-on courses organized by academic institutes (30.7%) or the Ontario Dental Association (22.9%); the least preferred training methods were online training modules and webinars (16.6% and 9.6%, respectively).
|
Barriers |
No. dentists (%) |
Facilitators |
No. dentists (%) |
|---|---|---|---|
| There is no separate code/fee associated with oral cancer exam. | 281 (30.4) | Availability of more efficient screening tools | 688 (75.2) |
| Professional dental organizations have not provided clinical guidelines for oral cancer exams. | 186 (20.2) | ||
| I am not comfortable palpating lymph nodes in a patient’s neck. | 120 (13.0) | Availability of less expensive screening tools | 672 (73.2) |
| Oral cancer examinations cause patients too much concern. | 118 (12.8) | ||
| Other dentists do not commonly provide routine oral cancer exams. | 112 (12.1) | More training on how to perform oral cancer exams | 647 (70.6) |
| I do not feel confident in my ability to perform an adequate oral cancer exam. | 85 (9.2) | ||
| I am uncomfortable discussing oral cancer risk factors with patients. | 84 (9.1) | A separate code in the suggested fee guide for oral cancer exams | 432 (47.1) |
| My knowledge about oral cancers is not current. | 79 (8.6) | ||
| A routine oral cancer exam is not necessary for each patient. | 75 (8.1) | More time available for patient exams | 429 (47.2) |
| Oral cancer exams require too much time. | 35 (3.8) |
Dentists’ Capacity to Prevent Oral Cancers
Identifying risk factors: Most dentists identified tobacco use (99.5%), heavy use of alcohol (97.2%), prior oral cancer lesions (98.6%) and a history of HPV infection (88.2%) as characteristics of patients at high risk for oral cancer. Fewer respondents identified older age (69.6%), male sex (45.4%) and low consumption of fruits and vegetables (31.8%) as potential risk factors.
Adequacy of relevant training for patient counseling: Most survey respondents reported feeling inadequately trained in oral cancer prevention. Smaller proportions of dentists either strongly agreed or agreed that they are adequately trained to provide tobacco cessation counseling (39.6%), recommend the HPV vaccine (29.5%) and provide counseling in alcohol cessation (22.3%).
Readiness of dentists to evaluate and discuss the risk: Large proportions of dentists regularly assess all or some of their patients’ histories of oral cancers (96.3%) and tobacco/alcohol use (98.0% and 85.1%, respectively) (Table 4). However, fewer dentists reported assessing patients’ histories of sexually transmitted infections (67.6%) and, specifically, HPV infections (51.9%). Approximately 21.0% of dentists surveyed reported asking about HPV vaccine status among all or some of their patients. Nearly 97% of respondents said that they discuss tobacco use and oral cancer incidence with all or some of their patients, while 84.4% reported discussing the link between oral cancer and alcohol use. In contrast, 47.2% of respondents said they discuss with all or some of their patients the link between HPV infection and oral cancer.
|
Action Stage |
Pre-Action Stage |
|||
| Practice | Yes, with all patients, no. (%) | Yes, but only with some patients, no. (%) | No, but I have thought about it, no. (%) | No, and I have no plans to start, no. (%) |
|---|---|---|---|---|
| Note: HPV = human papilloma virus. | ||||
| Assess patient’s alcohol use | 624 (67.5) | 163 (17.6) | 104 (11.2) | 34 (3.7) |
| Assess patient’s tobacco use | 831 (89.8) | 76 (8.2) | 11 (1.2) | 7 (0.8) |
| Assess patient’s sexually transmitted infection history | 512 (55.4) | 113 (12.2) | 204 (22.1) | 96 (10.4) |
| Assess patient’s history of HPV infection | 354 (38.5) | 123 (13.4) | 340 (37.0) | 102 (11.1) |
| Assess patient’s HPV vaccination status | 112 (12.2) | 82 (8.9) | 559 (60.8) | 167 (18.2) |
| Assess patient’s history of oral cancer | 805 (87.3) | 83 (9.0) | 24 (2.6) | 10 (1.1) |
| Discuss the connection between alcohol and oral cancer with patients | 242 (26.2) | 537 (58.2) | 116 (12.6) | 28 (3.0) |
| Discuss the connection between tobacco and oral cancer with patients | 406 (43.9) | 489 (52.9) | 24 (2.6) | 5 (0.5) |
| Discuss the connection between HPV and oral cancer with patients | 115 (12.5) | 320 (34.7) | 418 (45.4) | 68 (7.4) |
Factors affecting the readiness of dentists to discuss the risk factors with patients: Logistic regression analyses were conducted to assess characteristics predicting dentists’ readiness to discuss 3 major oral cancer risk factors with their patients, namely, smoking, alcohol use and HPV infection (Table 5). The findings indicate that readiness to discuss tobacco use and oral cancers does not differ with sociodemographic characteristics. However, age, gender, practice type and perception of alcohol as a risk factor are significant predictors of dentists’ readiness to discuss heavy alcohol use and oral cancer risk with patients. …